Recent falls in age-specific estimates of the case fatality ratio in England
February 11, 2021
Daniel Howdon, Jason Oke, Carl Heneghan
We present estimates of age-specific case fatality ratios in England. Recent weeks have seen falls, particularly concentrated in 80+ age groups. While results are consistent with the impact of disproportionate vaccination of these groups, we can only point tentatively towards such an effect.
Previous work has examined trends over time in the case fatality rate (CFR) for England. We extend this work by applying the same method to data as of 9 February 2021 in order to obtain age-specific estimates. These estimates exhibit large falls in recent weeks, particularly in the 80+ population that was first prioritised for vaccination.
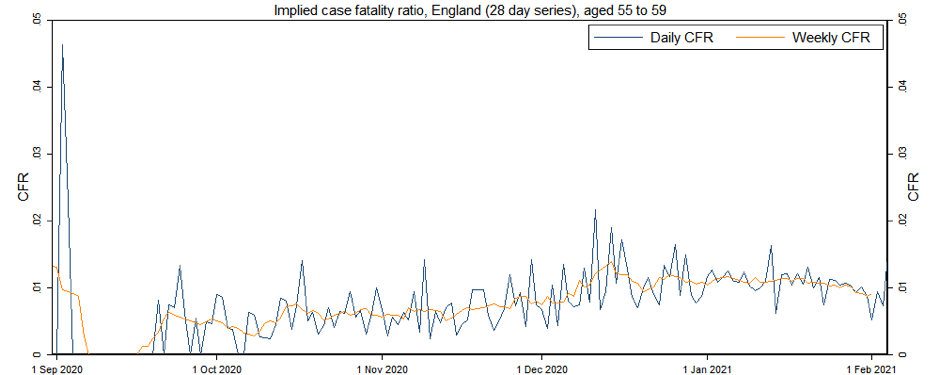
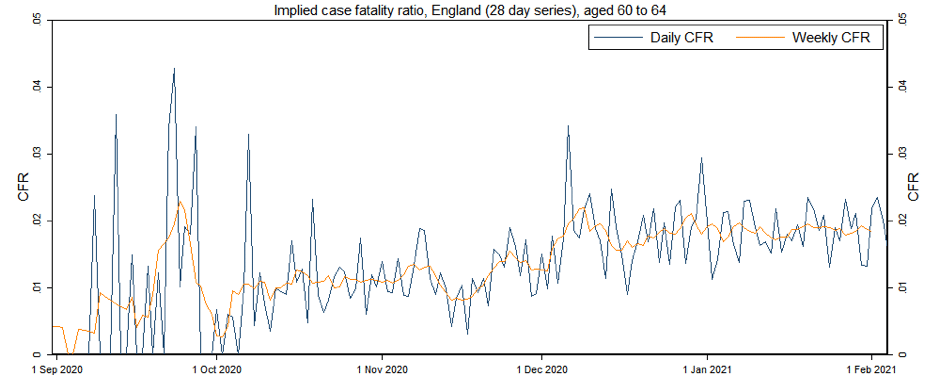
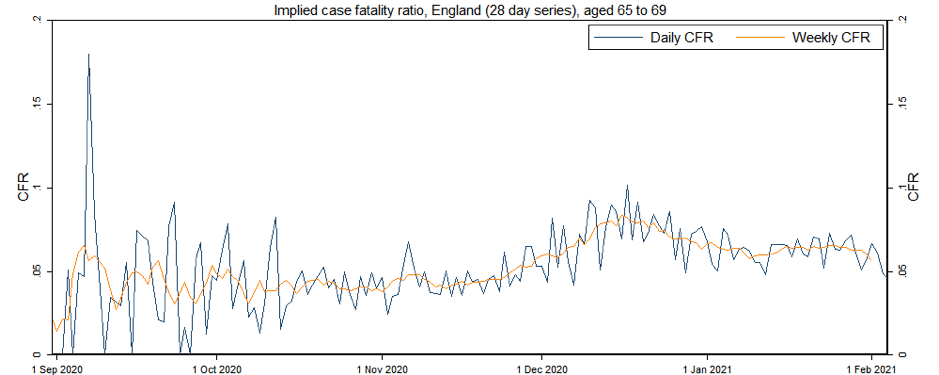
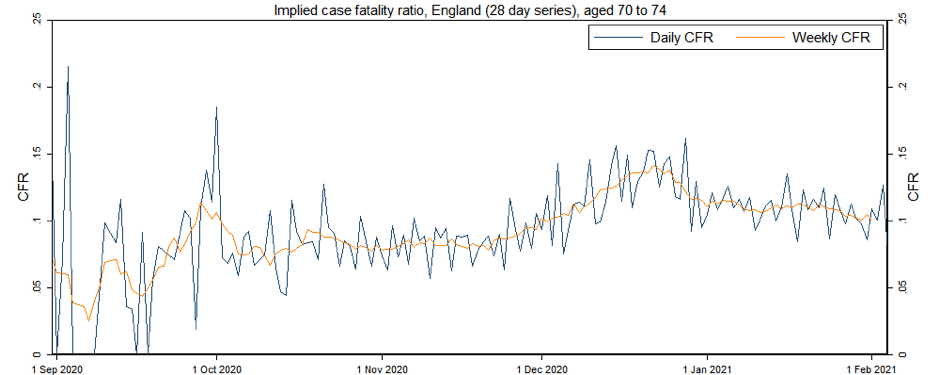
We use age-stratified data from the COVID-19 Public Health England dashboard on deaths within 28 days of a positive test by date of death, and cases by date of specimen. We estimate weekly CFRs, showing the ratio of announced deaths to estimated cases at risk in rolling seven day periods.
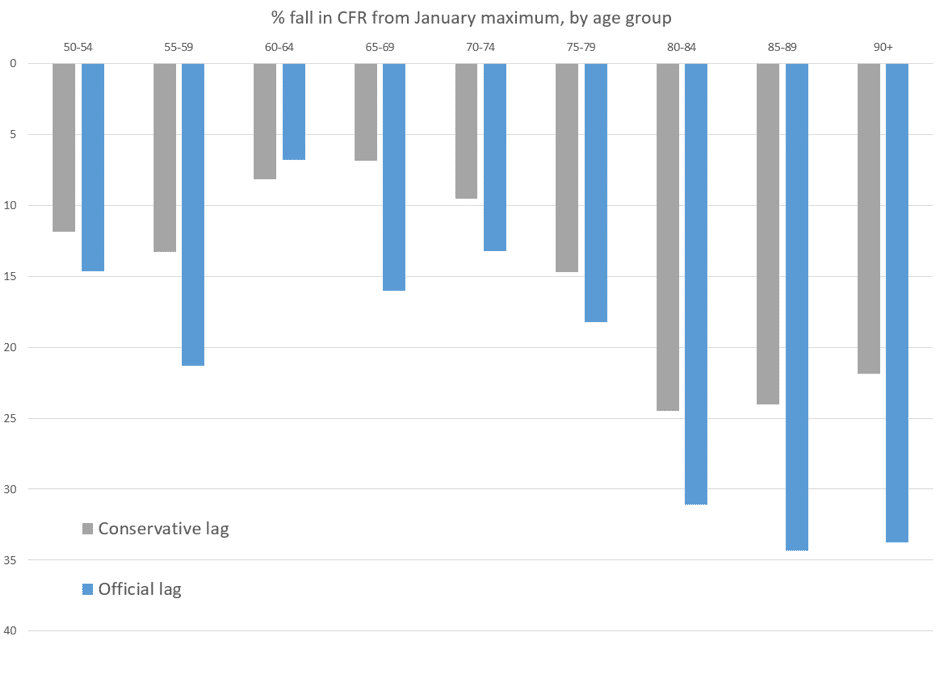
For each five year age group over 50, we present the maximum estimated weekly CFR observed in January, the most recent estimate of the CFR applying the official 5-day lag as proposed on the COVID-19 PHE dashboard, and a more conservative estimate adding on an extra 4 days to account for a potential increased recent lag. We observe falls in the CFR of over 30% for all 80+ age groups applying the official 5-day lag, and of over 20% applying an additional conservative 4-day lag.
| From age |
Max weekly CFR, January |
Conservative lag, weekly CFR |
Official lag, weekly CFR |
% fall in CFR from max (Conservative lag) |
% fall in CFR from max (Official lag) |
| 50-54 |
0.7% |
0.6% |
0.6% |
11.88 |
14.65 |
| 55-59 |
1.2% |
1.0% |
0.9% |
13.27 |
21.3 |
| 60-64 |
2.0% |
1.8% |
1.8% |
8.18 |
6.8 |
| 65-69 |
6.7% |
6.2% |
5.6% |
6.87 |
15.99 |
| 70-74 |
11.5% |
10.4% |
10.0% |
9.51 |
13.25 |
| 75-79 |
20.9% |
17.8% |
17.1% |
14.7 |
18.23 |
| 80-84 |
32.9% |
24.9% |
22.7% |
24.47 |
31.09 |
| 85-89 |
40.6% |
30.9% |
26.7% |
24.02 |
34.31 |
| 90-120 |
47.0% |
36.7% |
31.1% |
21.85 |
33.75 |
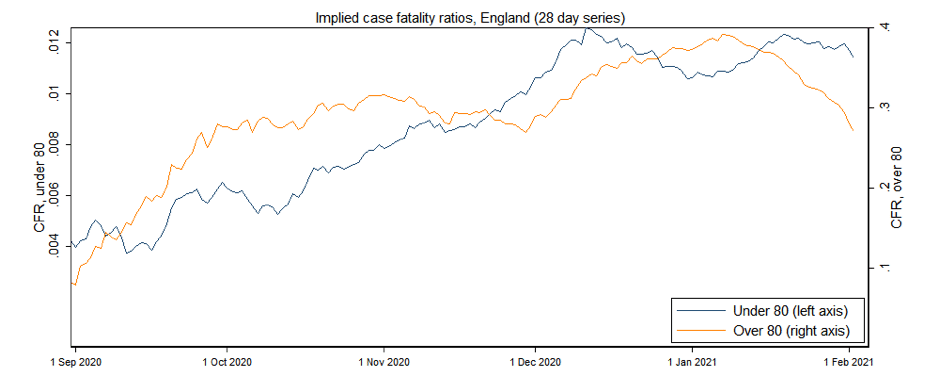
We also graphically present estimates of the CFR since September. We first show CFR estimates for those aged under 80, and for those aged 80 and above. While estimates of the CFR over time have exhibited substantial variation, recent such estimates for over 80s have fallen sharply, unlike those for the under 80 age group.
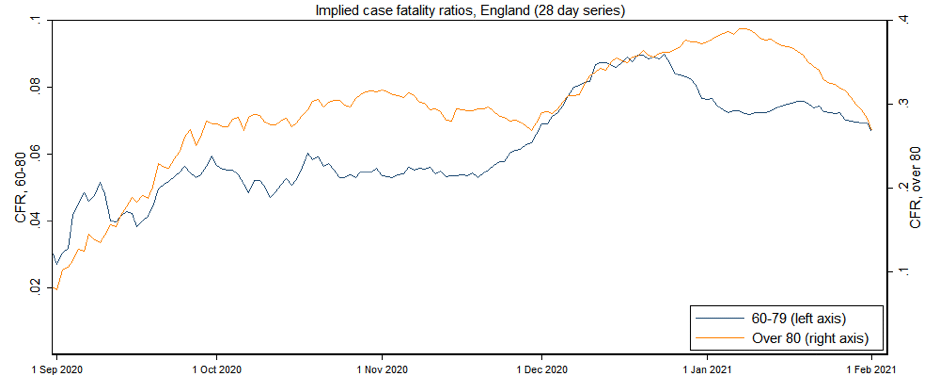
In order to check for similar patterns in groups closer in age, we also present estimates for those aged 60-79, and those aged 80 and above. Again, CFR estimates for over 80s have fallen substantially more sharply in recent weeks than for those in the 60-79 age group.
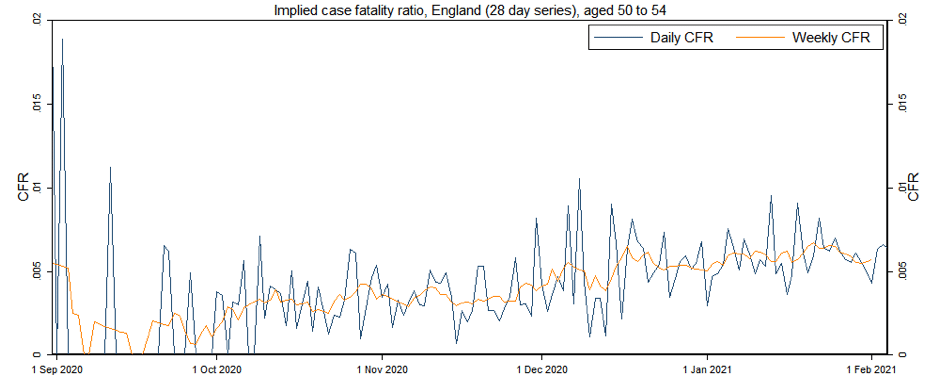
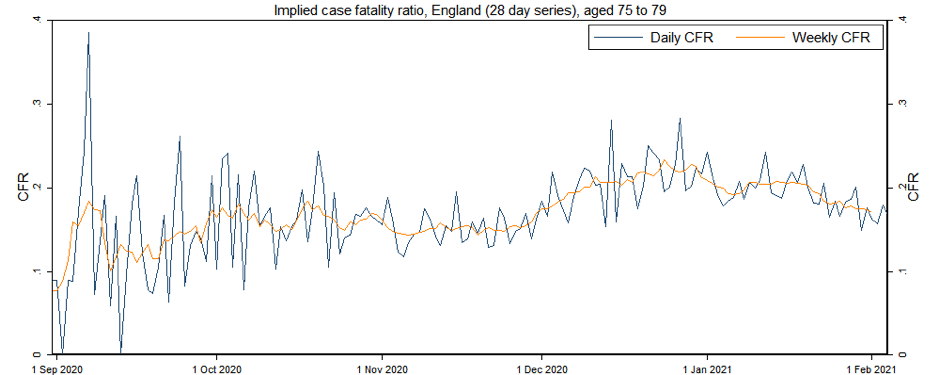
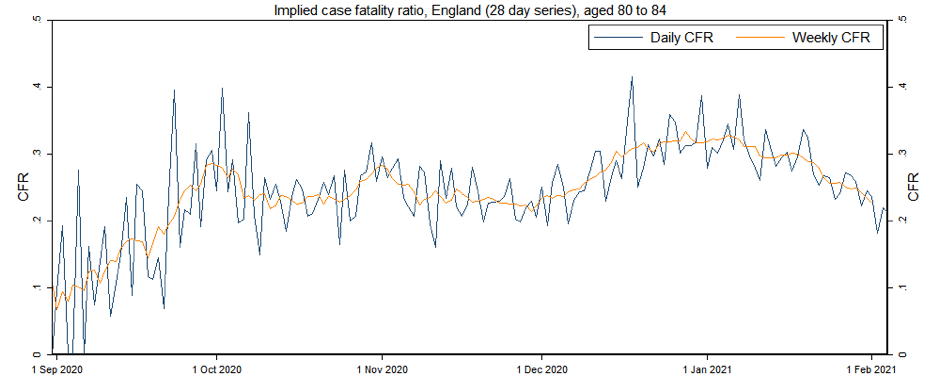
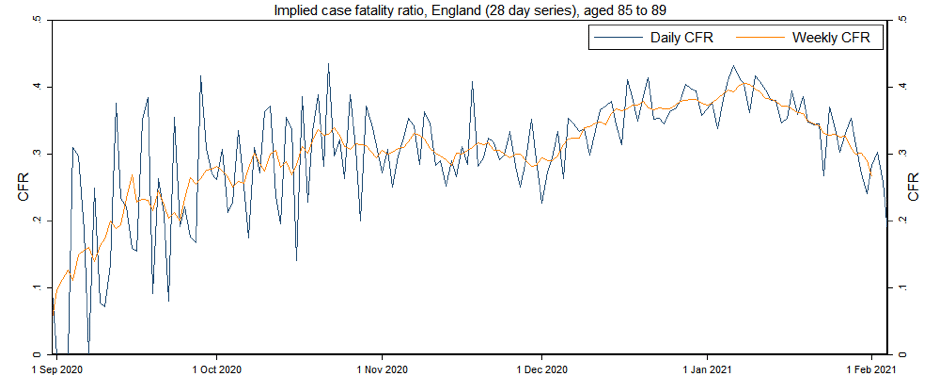
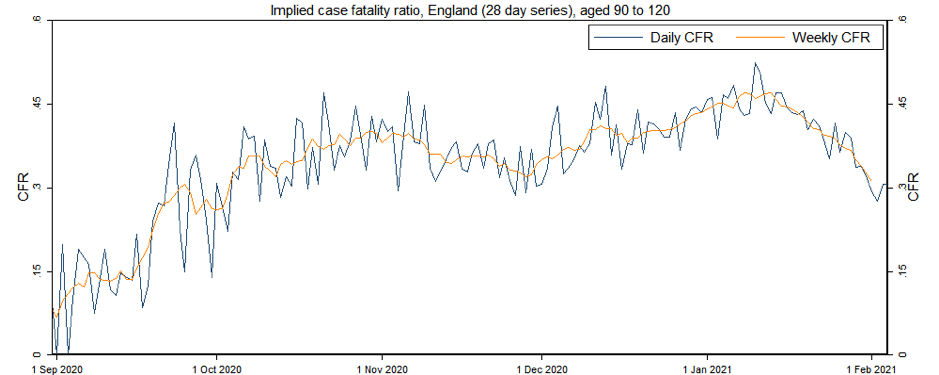
We finally break these CFR estimates down into five year age categories. These estimates again exhibit substantial variation over time, but with a sharp fall in recent CFR estimates for more heavily vaccinated age groups. The 90+ age group in particular exhibits a most recent estimate of the CFR that was last as low on 4 October (applying official lags) or 6 October (applying our more conservative lag).
While several explanations are possible for these patterns (see limitations section), these results do point to a potential impact of vaccination on the CFR for 80+ age groups. A fall in the CFR would be expected if vaccination reduces the post-infection probability of death to a greater extent than the probability of being determined to be a case.
Limitations and caveats:
While the use of deaths by date of death most accurately characterises the gap in time from case detection to death, the accurate reporting of deaths to recent days by this measure is subject to lags. While we attempt to overcome this by conservatively removing the most recent four days beyond this, this means not making use of most recent data. Trends using both measures are, however, clear, exhibiting much greater falls in the 80+ population.
The gap in time from case detection to death is likely to differ by age. To the best of our knowledge, no parametric estimates are available of this period.
While the 80+ population was prioritised for vaccination and was vaccinated in much greater proportion as a result, substantial numbers of the under 80 population have also been vaccinated. While this would tend to dampen down our ability to detect any impact, the much greater extent of vaccination among the 80+ population should still allow the detection of such an effect: as of 7 January, just over one month ago, official Public Health England figures show around 28% of the 80+ population to have been vaccinated compared to only 3% of the 75-79 population. Furthermore, smaller numbers of deaths in younger age groups may make more difficult the accurate estimation of the CFR for younger such groups.
Trends in the CFR also exhibit large variation over time. While this is partly an artefact of changes in testing behaviour, work on data in Florida and Australia, as well as in Europe, has pointed to potential seasonality of this CFR. Other factors behind such trends, such as pressures in hospital, are also likely to exist.
Daniel Howdon is a Senior Research Fellow in Health Economics, Leeds Institute of Health Sciences. Bio here
Jason Oke is a Senior Statistician at the Nuffield Department of Primary Care Health Sciences and Module Coordinator for Statistical Computing with R and Stata (EBHC Med Stats), and Introduction to Statistics for Health Care Research (EBHC), as part of the Evidence-Based Health Care Programme.
Carl Heneghan is Professor of Evidence-Based Medicine, Director of the Centre for Evidence-Based Medicine and Director of Studies for the Evidence-Based Health Care Programme. (Full bio and disclosure statement here)
Disclaimer: the article has not been peer-reviewed; it should not replace individual clinical judgement, and the sources cited should be checked. The views expressed in this commentary represent the views of the authors and not necessarily those of the host institution, the NHS, the NIHR, or the Department of Health and Social Care.