COVID-19 Registered Trials – and analysis

COVID-19 trials registered up to 8 March 2020—an analysis of 382 studies
Jeffrey K Aronson, Robin E Ferner, Nicholas DeVito, Carl Heneghan
Download COVID-19 registered trials—an analysis (1)
On 31 December 2019, China reported cases of pneumonia from a previously unknown coronavirus, 2019-nCoV, also called SARS-CoV-2. The disease it causes has been called COVID-19. The latest figures (17 March 2020) suggest that about 180,00 people have been infected worldwide, with about 7200 deaths. The World Health Organization (WHO) designated COVID-19 a “public health emergency of international concern” on 30 January and declared it a pandemic on 11 March.
COVID-19 should have come as no surprise. Gralinski and Baric, in a review in 2015 wrote: “The existence of novel bat SARS-like coronaviruses that also use bat, civet and human angiotensin 1 converting enzyme 2 (ACE2) receptors for entry, such as SARS-CoV [now SARS-CoV-1], strongly suggests an opportunity for further zoonotic disease outbreaks in human and animal populations.” Yet attempts to develop effective treatments against two other coronavirus diseases, SARS and MERS, have so far failed.
The coronaviruses are single-stranded RNA viruses that encode for four enzymes essential to the viral life cycle. They enter mammalian cells through an interaction of a viral spike glycoprotein and a receptor—ACE2 for SARS-CoV-1 and SARS-CoV-2 and dipetidylpeptidase 4 for MERS.
While the outbreak of COVID-19 was intensifying and spreading globally, 382 trials were registered between 23 January and 8 March (379 registered in China) on the WHO’s International Clinical Trials Registry Platform (ICTRP), some of which might affect morbidity and mortality and help us understand the disease.
We downloaded the listings of these 382 registered trials and classified them to aid interpretation of the type of interventions being proposed. The numbers of new trials that have been added to the list since the middle of January are shown in Figure 1.
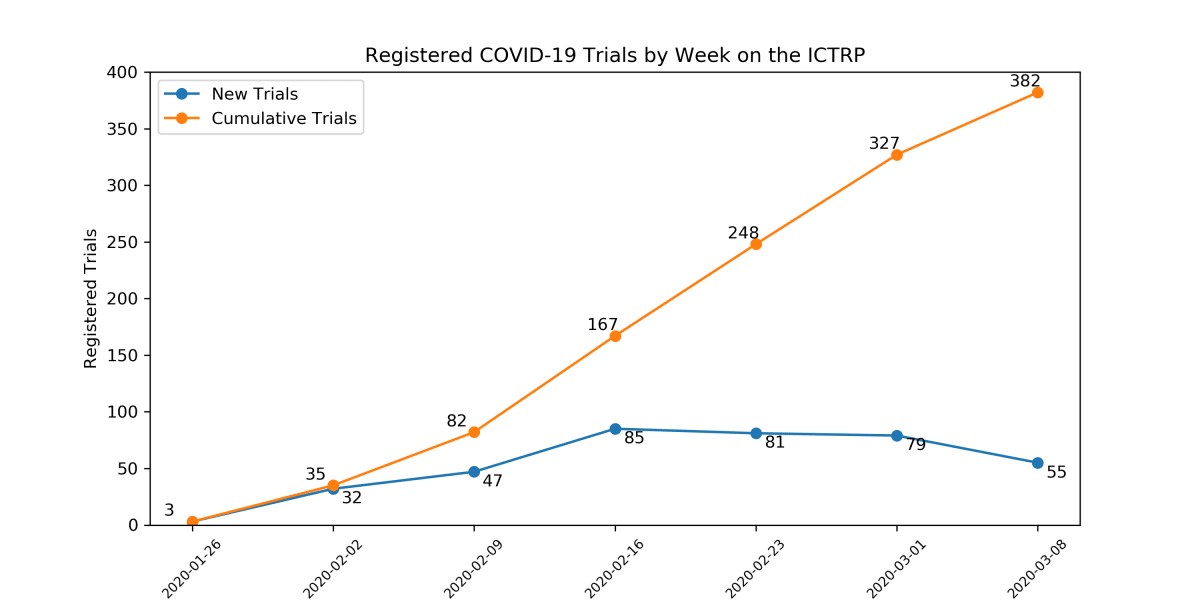
Figure 1. The numbers of new trials added to the WHO’s website week by week (blue), with the cumulative numbers (orange)
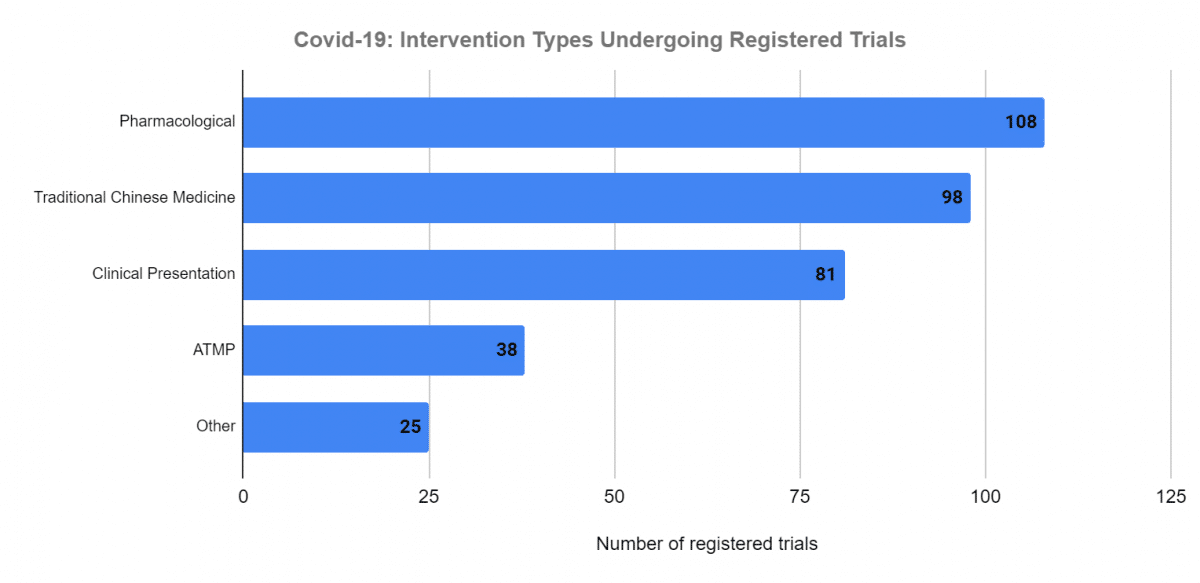
We categorized the 382 registered trials as follows (Figure 2):
- Pharmacological interventions, n = 108; see Table 1.
- Traditional Chinese Medicine (TCM), n = 98 (includes 48 named TCMs; 27 unspecified methods; 18 combinations with unspecified Western therapies; and 5 others, e.g. acupuncture).
- Clinical presentation, n = 81 (includes 63 studies of epidemiology, susceptibility factors, and clinical outcomes; 21 studies of diagnostic methods, both clinical and laboratory; and 19studies of prognostic features).
- Advanced therapy medicinal products (ATMP), n = 38, are medicinal products that include cellular therapies, tissue extracts, plasma, and vaccines for treatment not prevention. See the box at the end of the article for the 24 different interventions under investigation, the most common being mesenchymal stem cells and infusion of plasma from patients who have recovered (5 registered trials each).
- Others, n = 33 (includes nutritional supplements and enteral feeds; physiotherapy and exercise; physical therapies, such as renal replacement therapy; and psychotherapies).
- Two registered trials have been cancelled.
Proposed pharmacological interventions
Several agents may act directly against coronaviruses. Others, particularly monoclonal antibodies, may limit the cytokine dysregulation that causes fatal respiratory disease. Others may provide symptomatic relief.
In Table 1 we have listed the proposed pharmacological interventions and their mechanisms, when known, classified under 10 main headings (plus one heading to deal with combination studies):
- Antiviral drugs, not specified
- Antiviral drugs, broad spectrum
- Antiviral drugs, antiretrovirals
- Other antiviral drugs
- Antimalarial drugs
- Antibiotics and antiparasitics
- Nonspecific anti-inflammatory and immunosuppressive drugs
- Kinase inhibitors
- Monoclonal antibodies
- Miscellaneous others
Antiviral drugs that affect other RNA viruses (which include Ebola virus, rabies, influenza, hepatitis C, West Nile fever, polio, and measles), some of which have also been shown to have in vitro activity against 2019-nCoV, might be effective in COVID-19. However, in vitro activity of this sort does not guarantee clinical efficacy. Indeed, a note of caution is required. In experimental animals ribavirin, for example, enhanced the infectivity of SARS-CoV-1. Furthermore, in a systematic review of 30 trials of ribavirin in patients with SARS, 26 were classified as inconclusive and four showed possible harm. There is no guarantee that antiviral drugs will be beneficial in COVID-19, and adverse reactions are likely.
Antiviral drugs that are effective against DNA viruses, such as HIV, would not be expected to be as efficacious. Although some have been shown to be effective in vitro against 2019-nCoV, that is no guarantee of in vivo efficacy.
Chloroquine has been shown to be effective, both in vitro and clinically, against the coronavirus that caused SARS in 2003-4, SARS-CoV-1. Again, this does not predict clinical efficacy in COVID-19.
Corticosteroids may be harmful. In a systematic review of 29 low-quality studies of steroid use, 25 were inconclusive and in four there was evidence of harm. A further evidence review did not support corticosteroid treatment, reporting no evidence of net benefit with corticosteroids in “respiratory infection due to RSV, influenza, SARS-CoV [SARS-CoV-1], or MERS-CoV”, and showing that corticosteroids probably impair clearance of SARS-CoV-1.
As far as the miscellaneous group of other medicines is concerned, there are mechanistic arguments in favour of some of them and not others. For example, there is no good evidence that vitamin C is efficacious in treating any condition other than vitamin C deficiency; furthermore, the pharmacokinetics of vitamin C are such that the administration of even very high oral doses does not increase the body load, as reflected by plasma concentrations, by more than twofold and can cause diarrhoea and renal stones, since its absorption from the gut is saturable and it has high renal clearance.
Table 1. Medicines that are currently undergoing clinical trials or have trials planned in the management of COVID-19, due to the single-stranded RNA virus 2109-nCoV (SARS-CoV-2)
|
Type of medicine |
Mechanism of action |
No. of trials |
| Antiviral drugs, non-specific |
| Immunoglobulin |
Contains nonspecific antibodies; proposed to block viral Fc receptor activation by boosting endogenous neutralizing antibodies and preventing antibody-dependent enhancement of infection |
1 |
| Interferons |
Activate cytoplasmic enzymes affecting viral messenger RNA translation and protein synthesis; evidence of minor efficacy in MERS-CoV in combination with ribavirin |
4 |
| Interleukin-2 |
Multiple anti-inflammatory actions |
1 |
| Antiviral drugs, broad spectrum |
|
| Favipiravir |
Inhibitor of viral RNA-dependent RNA polymerase; typically used in treating influenza, but inhibits the polymerase of other viruses in vitro (Ebola, yellow fever, chikungunya, norovirus, and 2019-nCoV) |
4 |
| Triazavirin |
Non-nucleoside antiviral drug; effective against tick-borne encephalitis virus and forest-spring encephalitis virus |
1 |
| Umifenovir |
Membrane haemagglutinin fusion inhibitor in influenza viruses; active against influenza virus infections, in which it may reduce the risk of bacterial pneumonia |
5 |
| Antiviral drugs, antiretrovirals |
|
| ASC09 |
HIV protease inhibitor; to be used in combination with ritonavir |
4 |
| Azvudine |
Azidocytidine nucleoside analogue; HIV reverse transcriptase inhibitor |
4 |
| Danoprevir |
Hepatitis C virus NS3 protease inhibitor; to be used in combination with ritonavir |
1 |
| Darunavir |
HIV protease inhibitor; used in combination with cobicistat, a CYP3A inhibitor |
2 |
| Lopinavir + ritonavir |
Both HIV reverse transcriptase inhibitors; ritonavir is mainly used to enhance the action of other drugs by inhibition of CYP3A4; in vitro and possible clinical efficacy in SARS-CoV |
2 |
| Remdesivir |
Nucleotide analogue; inhibitor of RNA-dependent RNA polymerase; used to treat Ebola and Marburg viruses; effective in vitro against SARS-CoV-1 and MERS and blocks infection with 2019-nCoV in vitro |
2 |
| Other antiviral drugs |
| Baloxavir marboxil |
Inhibitor of influenza virus cap-dependent endonuclease; to be combined with favipiravir or lopinavir/ritonavir |
2 |
| Antimalarial drugs |
| Chloroquine and hydroxychloroquine |
In addition to its antimalarial actions, chloroquine has some efficacy in HIV-AIDS and blocks infection by 2019-nCoV in vitro, perhaps by inhibiting glycosylation of viral ACE-2 or inhibition of quinone reductase 2, reducing synthesis of viral sialic acid; in one study to be combined with lopinavir/ritonavir |
23 |
| Dihydroartemisinin |
Interaction between its peroxide bridge and haem iron may underlie its antimalarial action; mechanisms of action against viruses, eg. zika virus, are not well understood; to be combined with the antimalarial drug piperaquine |
1 |
| Antibiotics and antiparasitics |
| Carriomycin |
A polyether antibiotic; monovalent cation selective ionophore; active against Gram-positive bacteria, mycoplasma; fungi, and yeasts |
2 |
| Suramin sodium |
Antiparasitic; mode of action not known; used to treat first-stage African trypanosomiasis and onchocerciasis |
1 |
| Nonspecific anti-inflammatory and immunosuppressive drugs |
| Corticosteroids |
Many anti-inflammatory actions; experience with corticosteroids in other infectious diseases has not been uniformly beneficial; in SARS corticosteroids may worsen the disease |
6 |
| Fingolimod |
Immunosuppressant; sphingosine 1-phosphate receptor modulator; used in multiple sclerosis |
1 |
| Leflunomide |
Immunosuppressant; thalidomide analogue; inhibitor of dihydro-orotate dehydrogenase and tyrosine kinases; causes degradation of intracellular transcription factors; used to treat rheumatoid arthritis and psoriatic arthritis |
1 |
| Thalidomide |
Immunosuppressant; mode of action poorly understood; inhibits production of excess tumour necrosis factor-alfa (TNF-α), down-regulates cell surface adhesion molecules involved in leukocyte migration, has anti-angiogenic activity, and modulates the thalidomide-binding protein, cereblon, mediating protein degradation; used to treat multiple myeloma |
2 |
| Kinase inhibitors |
| Jakotinib hydrochloride |
[Chinese literature only]; presumed inhibitor of Janus-associated kinases |
1 |
| Ruxolitinib |
Inhibitor of Janus-associated kinases (JAK1 and JAK2); used to treat myelofibrosis, polycythaemia vera, and graft-versus-host disease; to be combined with mesenchymal stem cell infusion |
1 |
| Monoclonal antibodies; to be used in combination with protease inhibitors |
2 |
| Adalimumab |
Target: TNF-alfa; used to treat rheumatoid arthritis, juvenile idiopathic arthritis, ankylosing spondylitis, psoriatic arthritis, psoriasis, hidradenitis suppurativa, Crohn’s disease, ulcerative colitis, and uveitis |
1 |
| Camrelizumab |
Target: receptors for programmed cell death protein 1 (PD-1); used in China to treat Hodgkin’s lymphoma and nasopharyngeal carcinoma, alone or in combination with gemcitabine + cisplatin |
1 |
| Eculizumab |
Target: C5 complement; used to treat paroxysmal nocturnal haemoglobinuria, atypical haemolytic uremic syndrome, refractory generalized myasthenia gravis, and neuromyelitis optica spectrum disorder |
1 |
| Mepolizumab |
Target: interleukin-5 (IL-5); used to treat eosinophilic asthma |
1 |
| PD-1 mAb |
Target: receptors for programmed cell death protein 1 (PD-1) |
1 |
| Tocilizumab |
Target: soluble and membrane-bound IL-6 receptors (sIL-6R and mIL-6R); used to treat rheumatoid arthritis, systemic juvenile idiopathic arthritis, juvenile idiopathic polyarthritis, giant -cell arteritis, and chimeric antigen receptor (CAR) T cell-induced severe or life-threatening cytokine release syndrome |
2 |
| Miscellaneous others |
| Acetylcysteine |
Mucolytic; symptomatic relief; oral N-acetylcysteine ameliorated the intestinal effects of porcine epidemic diarrhea coronavirus in piglets |
1 |
| Angiotensin receptor blockers |
Antagonists at angiotensin receptors (see ACE inhibitors) |
1 |
| Angiotensin converting enzyme (ACE) inhibitors |
To be used in at least one study in individuals with hypertension in addition to COVID-19; ACE-2, which facilitates the entry of 2019-nCoV into cells is not inhibited by ACE inhibitors |
1 |
| Bismuth potassium citrate |
Inhibits growth of Helicobacter pylori; used in peptic ulceration; may inhibit SARS-CoV1 helicase |
1 |
| Bromhexine hydrochloride |
Mucolytic; symptomatic relief; small trials in other respiratory disorders show only modest benefit. |
1 |
| Diammonium glycyrrhizinate |
Derivative of glycyrrhetinic acid used in Chinese medicine; a competitive inhibitor of high mobility group box-1; causes moderate inhibition of the porcine epidemic diarrhea coronavirus in vitro, with inhibition of entry of the virus into Vero cells and replication |
2 |
| Dipyridamole |
Antiplatelet action by inhibition of adenosine uptake; also inhibits cGMP-phosphodiesterase, augmenting the increase in cGMP produced by EDRF (endothelium-derived relaxing factor, nitric oxide); there is a suggestion that antiplatelet agents, including dipyridamole, slow the progress of idiopathic pulmonary fibrosis. |
1 |
| Ebastine |
Histamine H1 receptor antagonist (antihistamine); presumably intended for symptomatic relief |
1 |
| Hydrogen peroxide |
Non-specific supposed antiviral action in the throat |
1 |
| Inhaled gases |
Oxygen, hydrogen, or the combination; symptomatic relief of hypoxia by oxygen; molecular hydrogen is proposed to have an anti-inflammatory effect. |
4 |
| Pirfenidone |
Various mechanisms proposed; reduces fibroblast proliferation, production of fibrosis-associated proteins and cytokines, and increased biosynthesis and accumulation of extracellular matrix in response to cytokine growth factors such as transforming growth factor-beta (TGF-β) and platelet-derived growth factor (PDGF); used to treat idiopathic pulmonary fibrosis |
1 |
| Polyinosinic-
polycytidylic acid |
Analogue of double-stranded RNA; reportedly has agonist actions at: toll-like receptors TLR-3; retinoic acid inducible gene I (RIG-I)-like receptors; and melanoma differentiation-associated gene 5 (MDA5); reduces the amount of mRNA in vitro in PK-15 cells infected with transmissible gastroenteritis coronavirus; used in China to treat tumours; to be used in combination with vitamin C |
1 |
| rhG-CSF |
Recombinant human granulocyte colony-stimulating factor; its counterpart, granulocyte macrophage-colony stimulating factor, directs the activation, proliferation, and differentiation of myeloid-derived cells and causes maturation of antigen-presenting cells, thus affecting adaptive immune responses; the 3C-like protease of SARS-CoV-1 reduces expression of granulocyte-macrophage colony-stimulating factor (GM-CSF) in transfected cells in vitro |
1 |
| Thymosin |
A group of polypeptides, initially isolated from the thymus. They are involved in T-cell differentiation. There have been trials of their use in cancer treatment, with little evidence of benefit. |
1 |
| Tranilast |
Tryptophan analogue; anti-allergic, inhibits NLRP3 in the inflammasome pathway; used to treat bronchial asthma, atypical dermatitis, allergic conjunctivitis, keloid, and hypertrophic scars |
1 |
| Vitamin C |
Antioxidant; no evidence to support purported efficacy in any condition other than vitamin C deficiency; very high doses can cause nephrolithiasis. |
3 |
| Combination studies not included above |
| Adamumab + tozumab |
Names not recognized; these may be adalimumab and tocilizumab (qqv) |
1 |
| Interferon α |
Combined with antiviral drugs (lopinavir/ritonavir, ribavirin, umifenovir) |
3 |
| Lopinavir/ritonavir |
Combined with other antiviral drugs (emtricitabine and tenofovir) |
2 |
|
|
|
To quote the conclusion of the authors of a recent Chinese systematic review of 75 trials listed on the Chinese Clinical Registration Center’s website and clinicaltrials.gov, “based on the poor quality and small sample size[s] and long completion period[s] [of the registered trials], we will not be able to obtain reliable, high-quality clinical evidence about COVID-19 treatment for quite a long time in the future”.
Advanced Therapy Medicinal Products under investigation (n=24) (wording taken from the titles of the registered studies)
- Aerosol inhalation of vMIP: viral macrophage inflammatory protein
- Ankylosaurus; M1 macrophages target
- Anti-2019-nCoV inactivated convalescent plasma
- Anti-SARS-CoV-2 inactivated convalescent plasma
- Biological preparation of human placenta
- Convalescent plasma treatment
- Cord blood mesenchymal stem cells
- Human menstrual blood-derived stem cells
- Immunoglobulin from cured patients
- Inactivated Mycobacterium vaccine
- Infusion of convalescent plasma
- Mesenchymal stem cells
- Mesenchymal stem cells exosomes atomization
- mRNA-1273
- NK cells
- Plasma treatment
- Recombinant cytokine gene-derived protein injection
- Regulating intestinal flora
- Therapeutic antibody from recovered novel coronavirus pneumonia patients
- Umbilical cord blood mononuclear cells
- Umbilical cord mesenchymal stem cells (hucMSCs)
- Umbilical cord Wharton’s Jelly derived mesenchymal stem cells
- Umbilical Cord(UC)-derived mesenchymal stem cells
- Washed microbiota transplantation
|
Carl Heneghan is the Editor in Chief BMJ EBM and Professor of EBM, Centre for Evidence-Based Medicine in the Nuffield Department of Primary Care Health Sciences, University of Oxford
Competing interests: CH has received expenses and fees for his media work. He holds grant funding from the NIHR, the NIHR School of Primary Care Research and the NIHR Oxford BRC. CH is also Director of CEBM, which jointly runs the EvidenceLive Conference with the BMJ and the Overdiagnosis Conference with international partners, based on a non-profit making model.
Jeffrey Aronson is a physician and clinical pharmacologist working in the Centre for Evidence-Based Medicine in the Nuffield Department of Primary Care Health Sciences, University of Oxford. He is an Associate Editor of BMJ EBM and a President Emeritus of the British Pharmacological Society.
Competing interests: JKA has written papers on the subject of clinical trials and has written papers and edited textbooks on clinical pharmacology, pharmacovigilance, and adverse drug reactions.
Robin Ferner is a clinical pharmacologist at the School of Clinical and Experimental Medicine, University of Birmingham
Competing interests: No competing interests
Nicholas J DeVito is a researcher at the EBM Datalab at the University of Oxford.
Competing interests: ND is employed on an LJAF grant and is a Naji Foundation Scholar at the University of Oxford.
Disclaimer: the article has not been peer-reviewed; it should not replace individual clinical judgement and the sources cited should be checked. The views expressed in this commentary represent the views of the authors and not necessarily those of the host institution, the NHS, the NIHR, or the Department of Health and Social Care. The views are not a substitute for professional medical advice.