Drug vignettes: Baricitinib
January 18, 2021
Robin E Ferner*†, Jeffrey K Aronson
On behalf of the Oxford COVID-19 Evidence Service Team
Centre for Evidence-Based Medicine
Nuffield Department of Primary Care Health Sciences
University of Oxford
*University of Birmingham
†University College London
Correspondence to r.e.ferner@bham.ac.uk
Introduction
Severe COVID-19 is characterized by lung damage, which can be associated with very high concentrations of circulating cytokines (cytokine storm), including interleukin-6 (IL-6). Baricitinib modulates the production of cytokines, and has therefore been suggested as a possible treatment for severe COVID-19.
Mechanism of action
Baricitinib (Olumiant®) is a small-molecule inhibitor of Janus kinases (JAKs). Cells interact with cytokines through receptors on the cell surface. When a cytokine binds to a receptor, a signal that alters events within the cell is transmitted to the interior of the cell through a pathway that includes JAKs and Signal Transducers and Activators of Transcription (STATs) (Figure 1). The STAT3 pathway amplifies IL-6 signals and leads to hyperinflammation. Baricitinib preferentially inhibits JAK1 and JAK2, and so inhibits the effect of the cytokine interleukin 6 (IL-6) on the STAT3 pathway. Baricitinib might also inhibit endocytosis of SARS-CoV-2 virus by an indirect interaction with the cell-surface angiotensin-converting enzyme 2 (ACE-2).
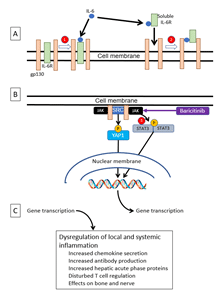
Figure 1. The mechanism of action of baricitinib
A. The interleukin-6 receptor (IL-6R) may be either membrane-bound or soluble
- In the classic pathway, IL-6 binds to membrane-bound receptor, which associates with the glycoprotein gp130; the gp130 dimerizes and initiates intracellular signalling.
- In the trans pathway, IL-6 binds to soluble IL-6R, which can also associate with gp130 and cause it to dimerize; (In a third mode of signalling, a dendritic cell presents receptor-bound IL-6 to gp130 on the surface of T-cells, leading to T-cell activation.
B. Dimeric gp130 activates JAK, which phosphorylates STAT3, and kinases of the SRC family, which phosphorylate the YES-associated protein-1 (YAP1); both STAT3 and YAP1 increase nuclear transcription of genes associated with inflammation. Baricitinib inhibits JAK1 and JAK2, and so interrupts the signal pathway; baricitinib inhibits JAK.
C. Increased transcription of genes associated with inflammation leads to increased cytokine storm and T-cell dysregulation.
[Based on Choy EH, De Benedetti F, Takeuchi T, Hashizume M, John MR, Kishimoto T. Translating IL-6 biology into effective treatments. Nat Rev Rheumatol 2020 Jun; 16(6): 335-45 and Garbers C, Heink S, Korn T, Rose-John S. Interleukin-6: designing specific therapeutics for a complex cytokine. Nat Rev Drug Discov 2018 Jun; 17(6): 395-412]
Indications for the licensed preparation
Baricitinib is presented as 2 mg and 4 mg tablets. It is licensed in the UK for treating rheumatoid arthritis and atopic dermatitis. For these indications it is recommended that it should not be started in patients with an absolute lymphocyte count less than 0.5 x 109/L, an absolute neutrophil count less than 1 x 109/L, or a haemoglobin less than 8 g/dL. It is contraindicated in pregnancy. Baricitinib has also been used to treat alopecia areata.
On 19 November 2020 the FDA issued an emergency use authorization (EUA) to Eli Lilly and Company for baricitinib, in combination with remdesivir, for treatment of suspected or laboratory confirmed COVID-19 in hospitalized adults and children two years of age or older requiring supplemental oxygen, invasive mechanical ventilation, or extracorporeal membrane oxygenation (ECMO).
Adverse effects
In its licensed indications, baricitinib is commonly or very commonly associated with the following adverse effects:
abnormal liver aminotransferases (transaminases);
headache;
Herpes zoster and Herpes simplex infections;
increased creatine kinase;
increased serum LDL cholesterol concentration;
nausea and abdominal pain;
rashes;
thrombocytosis;
upper respiratory tract infection.
More rarely, it has been associated with other adverse effects, including
diverticulitis;
hypertriglyceridaemia;
neutropenia;
thrombosis and thromboembolism;
urticaria;
weight gain.
Drug-drug interactions
Baricitinib is a substrate for the renal organic anionic transporter OAT3. Drugs that inhibit the transporter therefore reduce the elimination of baricitinib and increase exposure to it, as has been shown with probenecid, which increased exposure twofold. Care has also been recommended with teriflunomide, a metabolite of leflunomide.
Baricitinib in COVID-19
Animal experiments
In a study of SARS-CoV-2 infection in eight rhesus macaques, four were randomized to oral baricitinib 4 mg daily from 2 days after infection and four to no treatment. The animals were examined for 10 or 11 days before being sacrificed. Baricitinib was concentrated in the lungs (average post-mortem concentration over 4 micrograms/L; average blood concentration 2.13 micrograms/L). Viral RNA was detected in treated and control animals throughout the study, and both groups showed symptoms. Radiographs showed pulmonary infiltrates in 0/4 treated macaques and 2/4 untreated macaques; the latter also had higher serum concentrations of ferritin and CRP, markers of the severity of COVID-19 infection. Lung pathology, assessed by two pathologists who were masked to the treatments, was less severe in the baricitinib-treated monkeys. Genomic methods showed that baricitinib treatment suppressed the production of proinflammatory cytokines. The authors concluded that baricitinib might be beneficial in the treatment of COVID-19.
Clinical studies
Case reports
A 50-year-old man with a history of non-Hodgkin’s lymphoma became febrile, hypotensive, and tachypnoeic, with lymphopenia, a serum C-reactive protein concentration 20 times the upper limit of the reference range, and a CT scan showing alveolar interstitial thickness defined by ground-glass opacities with bilateral perihelia and peripheral distribution in combination with thickened interlobular and intralobular lines resembling an interstitial infection; a PCR test was positive in bronchoalveolar lavage fluid, although not on a throat swab. He was initially treated with baricitinib and then corticosteroids and tocilizumab, but continued to deteriorate. After remdesivir he showed signs of recovery. The authors interpreted the case as favouring tocilizumab and remdesivir, and commented that “early initiation of remdesivir may be effective in treating SARS-CoV-2.”
Observational studies
The effects of standard care plus baricitinib, 4 mg twice daily for 2 days then 4 mg daily for 7 days, have been studied in 20 patients with PCR-positive COVID-19 and evidence of pneumonia, for comparison with 56 patients with similarly severe COVID-19 who received standard care alone, which included either hydroxychloroquine, or lopinavir/ritonavir, or both. None received a corticosteroid. The dose of baricitinib was halved in patients over 75 years old.The outcomes favoured patients treated with baricitinib:
| |
Baricitinib, n = 20 |
No baricitinib, n = 56 |
| Mortality |
1 (5%) |
25 (45%) |
| Median CRP day 7 – day 0 |
–43.5 mg/L |
–26.5 mg/L |
| Incidence of adult respiratory distress syndrome (ARDS) |
3 (15%) |
15 (27%) |
| Median hospital stay |
12 days |
11 days |
Concentrations of IL-6 and TNF-alpha fell significantly more from day 0 to day 7 in the baricitinib-treated patients than in the controls.
The authors concluded that the “data suggest the potential effectiveness of short-term treatment with baricitinib for patients with ongoing SARS–CoV-2 infections in the absence of effective antiviral treatments or vaccines.”
In a pilot parallel group open study in 24 patients positive for SARS-CoV-2 with mild to moderate disease, 12 were treated with standard therapy, which included lopinavir/ritonavir plus baricitinib 4 mg/day for two weeks, and 12 were given standard therapy alone. The authors reported that they were encouraged by the results:
| |
Baricitinib, n = 12 |
No baricitinib, n = 12 |
| Cough after two weeks |
0 (0%) |
9 (75%) |
| Median temperature after 2 weeks |
36oC |
37.8oC |
| Median SpO2 after 2 weeks |
97% |
93.1% |
| Transfer to Intensive Care Unit |
0 (0%) |
4 (33%) |
| Discharged from hospital after 2 weeks |
7 (58%) |
1 (8%) |
The same authors reported a further series of adults with positive SARS-CoV-2 swabs and moderately severe pneumonia, of whom 113 received baricitinib and 78 hydroxychloroquine; both groups also received lopinavir/ritonavir:
| |
Baricitinib, n = 113 |
Hydroxychloroquine, n = 78 |
| Mortality |
0 (0%) |
5 (6.4%) |
| ICU admission |
1 (0.9%) |
14 (17.9%) |
| Discharged by end week 1 |
11 (9.7%) |
1 (1.3%) |
| Discharged by end week 2 |
88 (77.8%) |
10 (12.8%) |
| Median CRP day 14 – day 0 |
–79 mg/L |
–17 mg/L |
| Median Il-6 at week 2, pg/mL |
2.3 |
16.3 |
In an observational study patients with COVID-19 were given standard treatment, which included lopinavir/ritonavir, hydroxychloroquine, and in some patients intravenous immunoglobulin or interferon β-1b. If that was unsuccessful, they could receive methylprednisolone with or without one, two, or all of baricitinib, anakinra, and tocilizumab. The authors reported the outcomes in 62 patients who received methylprednisolone plus baricitinib (40 low-dose, 22 high-dose), compared with 50 who received methylprednisolone only. The primary endpoint was defined as the change in SpO2/FiO2 from hospitalization to discharge. Because patient characteristics differed between the study groups, the authors used propensity scores to adjust the results. The ratio of SpO2/FiO2 improved more in the patients who received baricitinib (mean adjusted difference +49; 95% CI = +22 to +77), and fewer baricitinib-treated patients required supplemental oxygen on discharge or one month later. Concentrations of D-dimers fell more in those who received baricitinib: –497 micrograms/L versus –269 micrograms/L (P=0.019). Mortality was not different between the two groups. Changes in SpO2/FiO2 were significantly greater in those who received high-dose baricitinib. As the authors commented, “results from randomized control clinical trials are indeed needed to confirm these preliminary results.”
There has been a brief report of data from the electronic healthcare records of 15 patients with PCR-positive COVID-19, who were treated “at the discretion of the medical team” with a combination of hydroxychloroquine plus baricitinib if they had evidence of pneumonia on lung imaging and required supplemental oxygen, or had raised inflammatory markers. Twelve of the patients recovered and three died. The authors encouraged a formal evaluation of JAK1/2 inhibitors in randomized controlled clinical trials.
Randomized trials
The ACCT-2 trial, a randomized, double-blind, placebo-controlled study in eight countries, reported outcomes in 515 patients treated with remdesivir + baricitinib, 200 mg on day 1 followed by 100 mg/day on days 2–10, and 518 treated with remdesivir + placebo. All the patients were in hospital with COVID-19. Baseline characteristics were similar in the two groups. The primary outcome measure was the time to recovery, with the day of recovery defined as the first day, during the 28 days after enrolment, on which a patient attained category 1, 2, or 3 on an eight-category ordinal scale. The median time to recovery was 7 days in the baricitinib group and 8 days in the placebo group (rate ratio for recovery = 1.16; 95% CI = 1.01 to 1.32; P = 0.03). In the subgroup who received high-flow oxygen or non-invasive ventilation, the rate ratio for recovery was 1.51 (95% CI = 1.10 to 2.08). The risk of death by 28 days was 5.1% in the baricitinib group and 7.8% in the placebo group (hazard ratio = 0.65, 95% CI = 0.39 to 1.09). Serious adverse events occurred in both groups, but new infections—a potentially important danger of immune modulators—occurred less often in the baricitinib group than in the control group. The authors concluded that “baricitinib plus remdesivir was superior to remdesivir alone in reducing recovery time and accelerating improvement in clinical status, notably among patients receiving high-flow oxygen or non-invasive mechanical ventilation. The combination was associated with fewer serious adverse events.”
Registered clinical trials
We are currently aware of 16 clinical trials involving baricitinib in 9447 patients; 11 are stated to be randomized, involving 8342 patients (83%); four are stated to be double- or triple-masked, involving 4144 patients (44%). Only three have mortality as an endpoint; of those, all three are randomized but only one is also double-masked.
Outlook
The results of the single randomized trial so far reported show modest benefit only, as patients treated with baricitinib plus remdesivir recovered one day sooner than those treated with remdesivir alone. There was no significant difference in overall mortality. It may be that patients who are seriously ill in the later stage of COVID-19, with very high circulating cytokine concentrations, will benefit most from this JAK1/2 inhibitor, but that has yet to be demonstrated convincingly. Targeting a single aspect of the immune response in severe COVID-19 may not be as effective as targeting multiple aspects, for example using corticosteroids.