COVID-19 – Collateral Damage in Scotland
April 24, 2020
Jason Oke, Carl Heneghan
The term collateral damage refers to any death, injury, or other damage as an unintended result of military operations. It is not a pleasant concept but one that has now been used in the context of COVID-19 and the side-effects of the lockdown.
Professor Sikora warned this week that screening and delays in diagnosis and cutbacks to cancer treatment could lead to excess cancer deaths as a result of the pandemic. If the lockdown means those who most need medical help don’t seek it – either because they can’t or are reluctant too will inevitably result in avoidable deaths.
Up to now, it has been difficult to quantify the recess deaths by the underlying cause but a recent data release from National Records of Scotland allows us to look at this in more detail.
In this dataset, deaths are broken down by underlying causes along with a reference point – the average of the last five years. This average means we can compare what is happening now with what we could expect.
The figure shows time series of excess deaths for cancer, dementia, circulatory diseases, respiratory and “other” causes from week 1 (week ending 3rd Jan) to week 16 (week ending 17th April).
Excess is defined as the difference between the deaths registered in 2020 and the average deaths over the preceding five-years. We calculated the standard deviation of excess for weeks 1 to 8 in order to define normal cause variation and then used this to form a threshold (3* standard deviations) that helps identify special cause variation. We also estimated the excess deaths per million population using an average of 5.454 million for Scotland and Mid 2018 averages data that reports 83% were adults (for cancer and cardiovascular disease excess deaths) and 19% were over 65 ( for Alzheimer disease excess deaths).
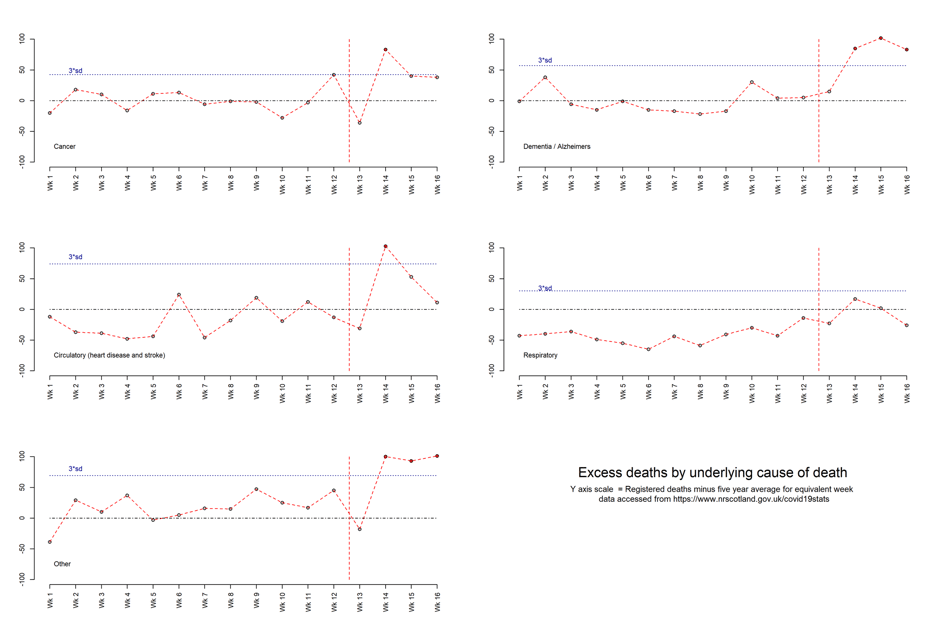
The data shows in week 14 significant increases corresponding to 38 extra cancer deaths (8.4 per million adults);103 circulatory deaths (22.8 per million adults) and 100 from other causes, and 83 extra dementia/Alzheimer’s deaths (80 per million adults over 65). There was no increase in respiratory deaths.
Whilst evidence of excess deaths continues for dementia/Alzheimer’s “other causes”, cancer and circulatory causes have returned to within the bounds of normal variation.
There are two possible explanations, either these deaths did not involve COVID-19 and result of the conditions brought about by the lockdown or COVID-19 was involved but not recognised and not recorded on the death certificate. Finally, it is worth noting that deaths from COVID-19 show that for weeks 14 (588) and 15 (637) people died in Scotland.
See also COVID-19: Activity in Scotland
AUTHORS
Jason Oke is a Senior Statistician at the Nuffield Department of Primary Care Health Sciences and Module Coordinator for Statistical Computing with R and Stata (EBHC Med Stats), and Introduction to Statistics for Health Care Research (EBHC), as part of the Evidence-Based Health Care Programme.
Carl Heneghan is Professor of Evidence-Based Medicine, Director of the Centre for Evidence-Based Medicine and Director of Studies for the Evidence-Based Health Care Programme. (Full bio and disclosure statement here)
Disclaimer: the article has not been peer-reviewed; it should not replace individual clinical judgement, and the sources cited should be checked. The views expressed in this commentary represent the views of the authors and not necessarily those of the host institution, the NHS, the NIHR, or the Department of Health and Social Care. The views are not a substitute for professional medical advice.