Does physical exercise prevent or treat acute respiratory infection (ARI)?
April 16, 2020
Marcy C. McCall, Carl Heneghan, David Nunan
On behalf of the Oxford COVID-19 Evidence Service Team
Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences,
University of Oxford
Correspondence to marcy.mccall@phc.ox.ac.uk
VERDICT
There is low quality evidence to suggest exercise has no impact on the rate and duration of acute respiratory infection but may provide a small reduction in severity of symptoms. Research in exercise immunology suggests moderate exertion may decrease the risk of acute respiratory infection in healthy adults but lacks assessment of its reliability. COVID-19 research would need to dedicate resources to robustly investigate exercise interventions as prevention or potential treatment during mild cases or to speed recovery from intensive care following ARI.
BACKGROUND
Of those patients who test positive for COVID-19, approximately 14% develop severe disease requiring hospitalisation and oxygen support and 5% require admission to an intensive care unit. 10% to 20% of severe patients develop acute respiratory distress syndrome (ARDS) during 8–14 days of the illness with complications including sepsis and septic shock, multiorgan failure, including acute kidney injury and cardiac injury (Yang et al, 2020). Older age and co-morbid disease (cardiovascular disease, diabetes, chronic respiratory disease, hypertension, cancer) are associated with higher mortality rates during COVID-19 infection.
Treatment Guidelines for COVID-19
There is no specific antiviral or other qualified treatment which has been proven effective for COVID-19.
The World Health Organization (WHO) interim guidance (13 March 2020) for clinical management COVID-19 recommend: symptomatic treatment in mild cases; oxygen therapy, monitoring, and treatment of co-infections in severe cases; and management for ARDS (mechanical ventilation), septic shock (vasopressor, resuscitation) and prevention of complications in critical cases. Physical exercise is not included as an intervention to avoid or promote during COVID-19 infection. In this rapid review, we ask what role, if any, should physical exercise play in the prevention or treatment of acute respiratory infection?
CURRENT EVIDENCE
Exercise and Acute Respiratory Infection (ARI)
In a Cochrane systematic review (updated 4 April 2020), authors analysed data (473 participants) from 14 trials (RCTs and quasi-RCTs) of participants age 18 to 85 years to evaluate effectiveness of exercise for altering the occurrence, severity, or duration of acute respiratory infections (ARIs). Main results of the study describe no observed difference between exercise and no exercise in the number of ARI episodes per person per year (risk ratio (RR) 1.00, 95% confidence interval (CI) 0.77 to 1.30; 4 trials; 514 participants; low‐certainty evidence); proportion of participants who experienced at least one ARI over the study period (RR 0.88, 95% CI 0.72 to 1.08; 5 trials; 520 participants; low‐certainty evidence); and symptom days per episode of illness (mean difference (MD) −0.44 day, 95% CI −2.33 to 1.46; 6 trials; 557 participants; low‐certainty evidence).
Exercise reduced the severity of ARI symptoms measured on the Wisconsin Upper Respiratory Symptom Survey (WURSS‐24) (MD −103.57, 95% CI −198.28 to −8.87; 2 trials; 373 participants; moderate‐certainty evidence) and the number of symptom days during follow‐up period (MD −2.24 days, 95% CI −3.50 to −0.98; 4 trials; 483 participants; low‐certainty evidence).
Exercise did not have a significant effect on laboratory parameters (blood lymphocytes, salivary secretory immunoglobulin, and neutrophils), quality of life outcomes, cost‐effectiveness, and exercise‐related injuries. There was no difference in participant dropout between the intervention and control groups. Certainty of evidence was low, downgraded by authors mainly due to limitations in study design and implementation, imprecision, and inconsistency.
In an overview (Rocco et al., 2018) researchers analysed data from four systematic reviews (including an older version of the Cochrane review; 14 primary studies) to examine clinical effectiveness of exercise to prevent upper respiratory tract infections. The authors were able to meta-analyse five randomized trials involving only 311 participants. They observed a reduction in incidence of infection (RR 0.84, 95% CI 0.65 to 1.10; 72 infections less [157 less to 45 more] per 1000 people) in people randomised or moderate intensity exercise for 8 weeks to 12 months. The evidence was judged “very low” quality based on GRADE, meaning the findings are highly uncertain.
Martin et al(2009) suggest outcomes following respiratory viral infections are improved after moderate exercise based on epidemiological evidence and animal models. They propose stress hormones stimulated during exercise reduce excessive local inflammation and skew the immune response away from a TH1 and toward a TH2 phenotype. Human studies and experimental modelling of mechanisms are lacking.
Exercise and Immunology
A 2020 systematic review (Gonçalves et al., 2020) included 15 small trials (8 RCTs, 7 non-RCTs) analysed acute (n=13) and chronic (n=2) aerobic exercise effects on inflammatory markers in healthy adult men and women (n=296, smallest n=8, largest n=64). Interventions ranged in intensity (60% to 85% VO2 Max) and duration of 18 to 240 minutes (n=14) or to exhaustion (n=1). None of the included studies were judged at low risk of bias for random allocation, selection bias, allocation concealment, blinding and selective reporting. Outcome measures attempted to understand the involvement of cells, immune cells, and binding molecules in short and long term exercise, and were listed as: Leukocytes, neutrophils and granulocytes; NK and NKT Lymphocytes and Cells: CD3+, CD4+, CD8+, CD16+, CD18+, CD19+, CD20+, CD22+, CD44+, CD45+, CD56+, CD95+, and their proportions; Cytokines and interleukins (IL): IL-1, IL-2, IL-6, IL-8, IL-10, and IL12; Tumor Necrosis Factor (TNF-α); Interferon-Gamma (IFN-γ); Immunoglobulin (Ig): IgG, IgA, and IgM; Adhesion Molecules: ICAM-1, ICAM-2, ICAM-3. No meta-analysis was attempted and tabulated vote-counting was used. The chronic effects of aerobic exercise on immunological markers remain equivocal and need further investigation in further studies.
A narrative review (Pederson & Toft, 2000) highlights evidence that exercise across a lifespan seems to increase resistance to upper respiratory tract infections, whereas repeated strenuous exercise suppresses immune function. There was no assessment of the reliability of data in the included studies. Elsewhere, Neiman concludes (2000, 1999, 1998, 1995) prolonged intense exercise causes immunosuppression, whereas moderate-intensity exercise improves immune function and potentially reduces risk and severity of respiratory viral infections. A J-shaped model depicts dose-dependent effect of exercise on risk and severity of respiratory tract infection (see Figure 1).
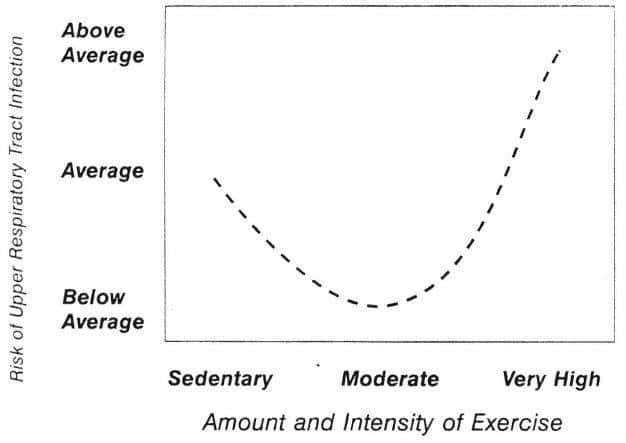
Figure 1. The J-shape of dose-response to exercise and respiratory tract infection (Copyright: Neiman 1999)
Research to support the J-shape dose-response was conducted in elite or trained athletes, limiting external validity of results. A positive response to moderate-exercise during acute respiratory illness appears unsubstantiated in other research, in populations where an exercise intervention could present serious adverse effects. In a more recent analysis, Neiman and Wentz (2019) summarise areas of exercise immunology, its progress and potential, advocating for new technology to answer existing questions on the interactions between exercise, nutrition, and immune function.
Exercise and ICU Recovery: Functional capacity and health-related quality of life
A nested cross-sectional study reported presence of inflammation after critical illness associated with poor physical recovery during the first 3 months post-intensive care unit (ICU) discharge. Skeletal function and muscular conditioning are additional benefits of regular exercise, especially following sedentary bouts of hospitalisation.
One systematic review of exercise-based rehabilitation trials (Connolly et al., 2015) following intensive care unit (ICU) discharge cited lack of methodological strength across studies and observed no discernable effect on functional capacity or health-related quality of life (HRQOL) after exercise interventions that were initiated during the post-ICU period.
EMERGING EVIDENCE IN COVID-19
Trials are ongoing to ascertain safe and effective interventions to reduce respiratory inflammation and infection caused by COVID-19. In 585 registered clinical trials (as of 16 April 2020), 12 prospective studies of COVID-19 include physical activity or exercise as a metric. Of these studies (n=7) plan to study exercise or meditation (n=1) intervention to improve stress or quality of life during social isolation. Two studies will observe COVID-19 effect on physical activity (Author 1: Ertürk, Turkey; Author 2: Avcil, Turkey). One study (Author: Péter, Hungary) will test efficacy of general health education (including physical activity advice) to decrease rates of hospitalisation and access to health services for COVID-19 disease. One listed study plans to implement a telerehabilitation program to COVID-19 patients measuring primary outcomes: VAS for dyspnea, Modified Borg scale for fatigue, Leicester Cough Questionnaire, Timed Up and Go,… (Author 1. Cirak, Turkey).
In summary, two of 585 registered trials (clinicaltrials.gov) aim to test effectiveness of exercise or physical activity for treatment of COVID-19 related symptoms.
CONCLUSIONS
There is low quality evidence to suggest exercise has no impact on the rate and duration of acute respiratory infection but may provide a small reduction in severity of symptoms. Research in exercise immunology suggests moderate exertion may decrease the risk of acute respiratory infection in healthy adults but lacks assessment of its reliability. COVID-19 research would need to dedicate resources to robustly investigate exercise interventions as prevention or potential treatment during mild cases or to speed recovery from intensive care following ARI.
End.
Disclaimer: the article has not been peer-reviewed; it should not replace individual clinical judgement and the sources cited should be checked. The views expressed in this commentary represent the views of the authors and not necessarily those of the host institution, the NHS, the NIHR, or the Department of Health and Social Care. The views are not a substitute for professional medical advice.
AUTHORS
Marcy C. McCall, BKin, MSc, DPhil, Departmental Lecturer and Senior Research Fellow, Nuffield Department of Primary Care Health Sciences
Carl Heneghan is Professor of Evidence-Based Medicine, Director of the Centre for Evidence-Based Medicine and Director of Studies for the Evidence-Based Health Care Programme. (Full bio and disclosure statement here)
David Nunan, BSc, MSc, PhD, Departmental Lecturer and Senior Research Fellow, Nuffield Department of Primary Care Health Sciences and Director of the Post Graduate Certificate in Teaching Evidence-Based Health Care
SEARCH STRATEGY
Rapid search strategy for current evidence conducted on MEDLINE, the Cochrane Library and Google Scholar (first 100 references). Terms: (((((“acute”[All Fields] OR “acutely”[All Fields]) OR “acutes”[All Fields]) AND ((((“respiratory tract infections”[MeSH Terms] OR ((“respiratory”[All Fields] AND “tract”[All Fields]) AND “infections”[All Fields])) OR “respiratory tract infections”[All Fields]) OR (“respiratory”[All Fields] AND “infection”[All Fields])) OR “respiratory infection”[All Fields])) OR ((((“virus diseases”[MeSH Terms] OR (“virus”[All Fields] AND “diseases”[All Fields])) OR “virus diseases”[All Fields]) OR (“viral”[All Fields] AND “infection”[All Fields])) OR “viral infection”[All Fields])) NOT (“hiv”[MeSH Terms] OR “hiv”[All Fields])) AND (((((((((((((“exercise”[MeSH Terms] OR “exercise”[All Fields]) OR “exercises”[All Fields]) OR “exercise therapy”[MeSH Terms]) OR (“exercise”[All Fields] AND “therapy”[All Fields])) OR “exercise therapy”[All Fields]) OR “exercise s”[All Fields]) OR “exercised”[All Fields]) OR “exerciser”[All Fields]) OR “exercisers”[All Fields]) OR “exercising”[All Fields]) OR (((“exercise”[MeSH Terms] OR “exercise”[All Fields]) OR (“physical”[All Fields] AND “activity”[All Fields])) OR “physical activity”[All Fields])) OR (“yoga”[MeSH Terms] OR “yoga”[All Fields])) OR ((((((((((“meditate”[All Fields] OR “meditated”[All Fields]) OR “meditating”[All Fields]) OR “meditation”[MeSH Terms]) OR “meditation”[All Fields]) OR “meditations”[All Fields]) ) OR “meditational”[All Fields]) OR “meditative”[All Fields]) OR “meditator”[All Fields]) OR “meditators”[All Fields])) AND ((“clinical trial”[Publication Type] OR “systematic review”[Publication Type]) OR “randomized controlled trial”[Publication Type])
SOURCES OF INFORMATION
All sources of evidence used in this review are available via the hyperlinks above.