Is a 14-day quarantine effective against the spread of COVID-19?
April 6, 2020
Marcy C. McCall, David Nunan, Carl Heneghan
On behalf of the Oxford COVID-19 Evidence Service Team
Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences
University of Oxford
Correspondence to: marcy.mccall@phc.ox.ac.uk
VERDICT
Effectiveness of quarantine during a viral outbreak relies on the timing and accuracy of the quarantine period, as well as the ability of individuals and health care providers to follow quarantine procedures. Current evidence to inform quarantine is limited, and COVID-19 infection trends raise critical questions about implementation effectiveness.
BACKGROUND
The COVID-19 pandemic of 2020 poses risks to physical health of those who contract the virus. At the time of writing, the number of confirmed cases just crossed the 1 million mark. On 22 March 2020, the World Health Organization (WHO) issued an updated document to encourage member-states to increase their level of preparedness for COVID-19.
Countries are advised to invoke strict quarantine procedures for individual cases of COVID-19. Countries experiencing clusters or a larger outbreak of the virus are encouraged to “implement all-of-society resilience, repurpose government, business continuity, and community services plans”. To date, over 80 countries have imposed travel bans or quarantine procedures by way of response to the COVID-19 insurgency.
What is a quarantine?
The concept of ‘quarantine’ is radically embedded in local and global health practices and culture, attracting heightened interest during episodes of perceived or actual epidemics.
According to the WHO, the quarantine of persons is the restriction of activities of or the separation of persons who are not ill but who may have been exposed to an infectious agent or disease, with the objective of monitoring their symptoms and ensuring the early detection of cases.
Quarantine is different from isolation, which is the separation of ill or infected persons from others to prevent the spread of infection or contamination. Introducing quarantine, according to the WHO: “aims to delay the introduction of the disease to a country or area or may delay the peak of an epidemic in an area where local transmission is ongoing, or both”.
Quarantine parameters for the COVID-19 virus include captivity that counts 2 days before and up to 14 days after the onset of the symptoms from a person with laboratory-confirmed disease. Countries have adapted this recommendation and will request travellers to observe a 14 day self-quarantine upon arrival from a foreign country.
The WHO guidance also recommends provisions of physical comfort including adequate ventilation, hygienic facilities, social distance of at least 1 metre between all persons quarantined, provision of food and water, access to internet, news and entertainment if possible, and psychosocial support must be made available.
For COVID-19, current research suggests that the typical incubation period is about five days and around 99% of the people who get infected and develop symptoms will do so within 14 days.
CURRENT EVIDENCE
A 2011 cross-sectional study on H1N1 examined quarantining practices and barriers to their effectiveness in Australia. In a sample of 297 participants, of the 90% of respondents who reported understanding what they were meant to do during quarantine, 55% (n = 147) reported full compliance. In contrast, full compliance was only reported by 35% (n = 11) of the minority who did not report that they understood what they were meant to do. Compliance was higher in the households that understood what they were meant to do (odds ratio 2.27, 95% CI 1.35-3.80).
An observational 2005 study on SARS concluded full-scale quarantine measures implemented in Taiwan led to a significant improvement in onset-to-diagnosis time of all patients. (1.2 days vs. 2.9 days for not quarantined).
In a 2001 review, physicians and scientists in the US weighed the potential benefit of a large-scale quarantine against the risk of bio-terrorism. Their findings advocate strategies other than quarantine would be more medically defensible, more likely to effectively contain the spread of disease, less challenging to implement, and less likely to generate unintended adverse consequences. Before invoking a quarantine, authors suggest asking:
- Do public health and medical analyses warrant the imposition of large-scale quarantine?
- Are the implementation and maintenance of large-scale quarantine feasible?
- Do the potential benefits of large-scale quarantine outweigh the possible adverse consequences?
In a rapid review (2020), authors analysed data from 14 studies to ascertain characteristics of adherence to quarantine procedures. Of nine studies reporting quantitative data, adherence rates of quarantined individuals ranged from 0% to 93%.
EMERGING EVIDENCE IN COVID-19
Recent modelling by Imperial College factored in household quarantine as a key intervention to mitigate against increased infection. Researchers defined a home-based quarantine in response to following identification of a symptomatic case in the household, where all household members remain at home for 14 days. Their assumption suggested household contact rates would double during the quarantine period, but contacts in the community would reduce by 75%, if 50% of each household comply with the policy.
The Italy case highlights, however, some challenges with the efficacy of current quarantine practices and the 14-day number. The Ministry of Health in Italy issued a press release Covid-19: “New mandatory quarantine measures and active surveillance” on 21st of February 2020. In addition, a nation-wide confinement came into effect on 8th of March 2020. The evolution of cases in Italy is still increasing (see Figure 1).
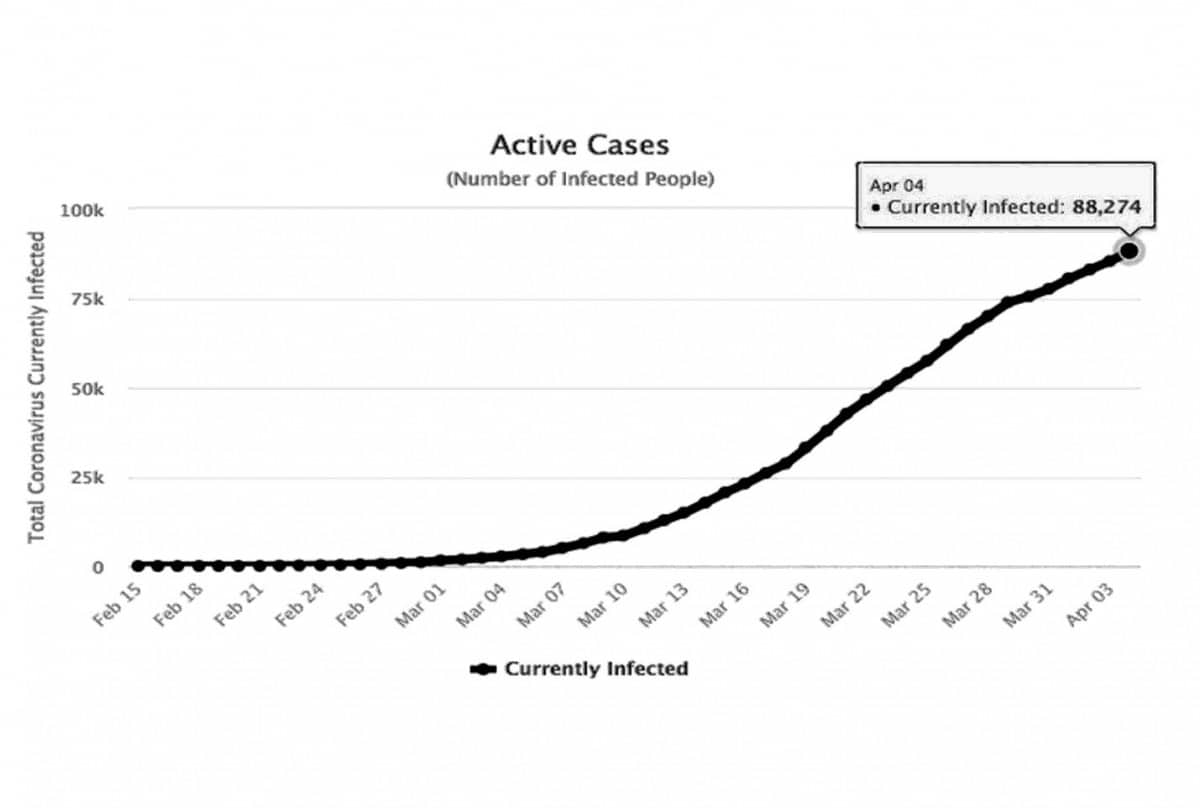
Figure 1. Active cases of COVID-19 in Italy
Image source: https://www.worldometers.info/coronavirus/country/italy/
In a recent paper, Italian physicians signalled concern over quarantining practices in healthcare facilities: “Hospitals are indeed a delicate place in epidemics: they collect fragile persons who can be exposed to the virus and are subsequently readmitted to the community thus spreading the infection.” The Italian-based authors express concern for the dearth of data to support the number of days for quarantine, and suggest there is added risk to infection of patients via respiratory equipment while in quarantine inside critical care units.
New case data: Italy, South Korea, and Sweden
If 14-day quarantine efforts are effective, the number of newly infected cases per day should slow two-weeks following the quarantine implementation. Current variation in testing practices, however, makes it impossible to understand if number of daily cases have peaked. Italy’s number of reported cases, as of 1st of April 2020. are at similar levels to 18th of March 2020 (see Figure 2).
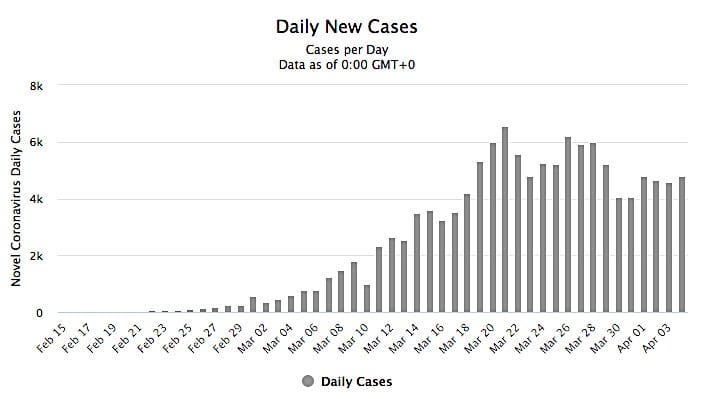
Figure 2. Number of newly daily cases of COVID-19 in Italy (2020)
Image source: https://www.worldometers.info/coronavirus/country/italy/
In South Korea, any national arriving from Wuhan region was required to observe a 14-day quarantine under strict surveillance. An internal policy of quarantine was on 26th of February, with a further amendment enforced on 3rd of March to allow the testing, quarantine and treatment of individuals suspected of having COVID-19, and if refused, would face prosecution. South Korea has also encouraged and made available rapid testing of the virus. On the 20th of March 2020, the country imposed testing to travellers arriving in the country from 22nd of March 2020; and a 14-day quarantine for any visitor arriving to South Korea as of 1st of April 2020. The case trajectory of South Korea (see Figure 3), indicates a surge of new cases during the week of February 27th to March 5th. A maintained reduction in new cases appears in South Korea from 11th of March 2020.
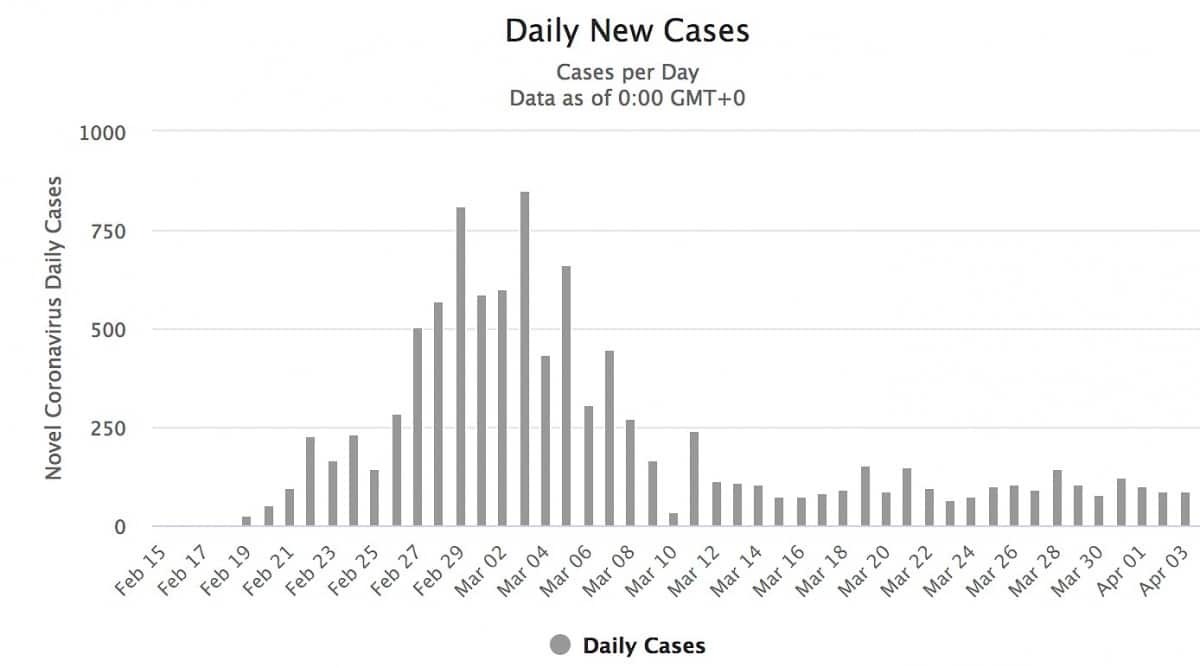
Figure 3. Number of newly daily cases of COVID-19 in South Korea (2020)
Image source: https://www.worldometers.info/coronavirus/country/south-korea/
In contrast to South Korea’s strict enforcement of quarantine with surveillance and rapid testing, the Swedish government issued a rules of conduct for residents and travellers, precluding health checks or quarantine measures to “avoid use of resources for little or no effect.”
As of 30th March 2020, the public health agency of Sweden recommends testing for two groups: hospitalised patients, or people that work in healthcare or elderly care, with suspected COVID-19. Health officials ask the public to reduce contact with others when ill and recommend self-treatment at-home if symptoms consistent with coronavirus appear. The daily new cases of COVID-19 in Sweden have declined from 621 to 312 from April 2nd to April 4th, 2020 (see Figure 4).

Figure 4. Number of newly daily cases of COVID-19 in Sweden (2020)
Image source: https://www.worldometers.info/coronavirus/country/sweden/
As countries respond to COVID-19, it is vital we conduct research in this current outbreak to address some of the unanswered questions on quarantine effectiveness, including: timing, implementation procedures, appropriateness, and cost-benefits.
Important limitations for readers: Epidemiological data for COVID-19 are highly variable and uncertain. Limited testing practices in several countries mean case numbers and infection rates could be underestimated or data skewed. (See: COVID-19 Case Fatality Rates)
CONCLUSION
Viruses don’t travel, people do. So intuitively, we expect that imposing physical space barriers will work to eradicate infection. However, the effectiveness of quarantine during a viral outbreak relies on the timing and accuracy of the quarantine period, as well as the ability of individuals and health care providers to follow quarantine procedures. The current evidence-base is limited, and COVID-19 infection trends raise critical questions about implementation effectiveness.
End.
Disclaimer: the article has not been peer-reviewed; it should not replace individual clinical judgement and the sources cited should be checked. The views expressed in this commentary represent the views of the authors and not necessarily those of the host institution, the NHS, the NIHR, or the Department of Health and Social Care. The views are not a substitute for professional medical advice.
SEARCH TERMS
Rapid search strategy conducted on MEDLINE, the Cochrane Library and Google Scholar (first 100 references). Terms: (“infect”[All Fields] OR “infectability”[All Fields]) OR “infectable”[All Fields]) OR “infectant”[All Fields]) OR “infectants”[All Fields]) OR “infected”[All Fields]) OR “infecteds”[All Fields]) OR “infectibility”[All Fields]) OR “infectible”[All Fields]) OR “infecting”[All Fields]) OR “infection s”[All Fields]) OR “infections”[MeSH Terms]) OR “infections”[All Fields]) OR “infection”[All Fields]) OR “infective”[All Fields]) OR “infectiveness”[All Fields]) OR “infectives”[All Fields]) OR “infectivities”[All Fields]) OR “infects”[All Fields]) OR “pathogenicity”[MeSH Subheading]) OR “pathogenicity”[All Fields]) OR “infectivity”[All Fields]) AND (“j rehabil assist technol eng”[Journal] OR “rate”[All Fields])) AND (((((“virally”[All Fields] OR “virals”[All Fields]) OR “virology”[MeSH Terms]) OR “virology”[All Fields]) OR “viral”[All Fields]) AND (((((“pandemic s”[All Fields] OR “pandemically”[All Fields]) OR “pandemicity”[All Fields]) OR “pandemics”[MeSH Terms]) OR “pandemics”[All Fields]) OR “pandemic”[All Fields]))) AND ((((“quarantine”[MeSH Terms] OR “quarantine”[All Fields]) OR “quarantines”[All Fields]) OR “quarantined”[All Fields]) OR “quarantining”[All Fields]) AND ((((“review”[Publication Type] OR “review literature as topic”[MeSH Terms]) OR “review”[All Fields]) OR ((“clinical trial”[Publication Type] OR “clinical trials as topic”[MeSH Terms]) OR “clinical trial”[All Fields])) OR “RCT”[All Fields]) OR ((((“cross-sectional studies”[MeSH Terms] OR (“cross sectional”[All Fields] AND “studies”[All Fields])) OR “cross sectional studies”[All Fields]) OR (“cross”[All Fields] AND “sectional”[All Fields])) OR “cross sectional”[All Fields])
SOURCES OF INFORMATION
All sources of evidence used in this review are available via the hyperlinks above.