Preventing non-COVID-19 hospital admissions during a pandemic: a rapid overview of the evidence for high-value medications
May 11, 2020
Niklas Bobrovitz*, Joseph Lee, Kamal R. Mahtani
On behalf of the Oxford COVID-19 Evidence Service Team
Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences
University of Oxford
*Faculty of Medicine, University of Toronto
*Massey College, University of Toronto
Correspondence to niklas.bobrovitz@mail.utoronto.ca; @nikbobrovitz
PDF to Download
VERDICT
Fourteen evidence-based, guideline-supported medications that significantly reduce emergency hospital admissions were identified. These apply to major chronic disease populations considered higher risk for COVID-19 morbidity and mortality. There is COVID-19 related guidance on optimising use of some of these medications, including indications for altering doses and taking mediation breaks. Health care practitioners and policy-makers should consider optimising therapeutic combinations and doses of these medications. Consideration may also be needed to adjust dispensing intervals to ensure that supplies are maintained, explore home delivery services, waive dispensing fees, and provide remote consultation support for patients to follow prescribed regimens.
BACKGROUND
To manage fluctuating surges in COVID-19 cases, the health system needs to increase acute care capacity. In addition to building temporary facilities and calling practitioners to the front line of care, capacity may be expanded by minimizing emergency care demands among non-COVID patients. This may be particularly relevant to non-COVID patients with long term conditions who, if admitted to hospital, may be at high-risk for hospital-acquired COVID-19 infection and a poor outcome.
Community-based practitioners may have existing strategies to prevent their patients from becoming acutely unwell and requiring hospital admission. However, the COVID-19 pandemic has disrupted routine healthcare provision and forced practitioners to prioritise their clinical activities. Therefore, the objective of this rapid review update was to identify a priority list of evidence-based medications for use in the community or emergency department that could prevent emergency hospital admissions among non-COVID patients.
SEARCHING FOR EVIDENCE
This was a rapid update of a previously published overview of systematic reviews. We searched for systematic reviews with meta-analyses of randomized controlled trials assessing medications in adults and reporting on emergency hospital admissions. To ensure we included only high value interventions with a significant evidence base we included medications if they met all of the following criteria:
- The medication had been directly compared to the standard of care, placebo, or no treatment (as defined by the original review authors) in a meta-analysis of randomised controlled trials;
- The meta-analysis evidence demonstrated a significant reduction (p<0.05) in emergency hospital admissions;
- The meta-analysis evidence for hospital admissions had been graded as moderate or high quality using Grading of Recommendations Assessment, Development and Evaluation (GRADE) Working Group criteria;
- The pooled effect estimates for hospital admissions had not been contradicted by other meta-analyses;
- The medications could be prescribed and administered in the community or an emergency department;
- Use of the medications was supported by NICE clinical guidelines.
We screened 12,107 titles/abstract and 1,830 full text articles. Of these, 163 systematic reviews were included for analysis – 23 were new reviews identified in the updated search. These reviews included hospital admissions data from over 700 RCTs and 600,000 participants.
Wherever possible, we included emerging evidence and guidance for optimising use of the medications in the context of the COVID-19 pandemic (i.e., medication safety, prescribing, dispensing, delivery, and adherence).
EVIDENCE FOR HIGH-VALUE MEDICATIONS
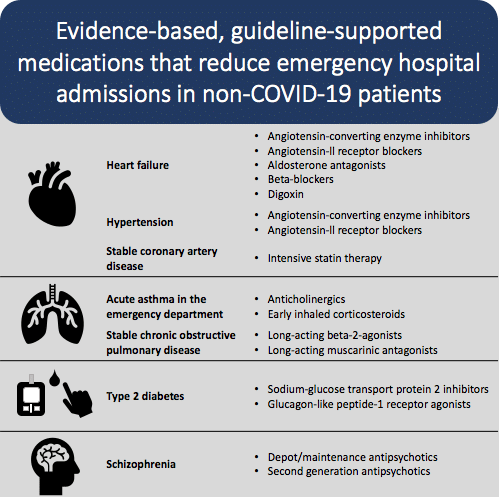
We identified 14 evidence-based and guideline-supported medications that significantly reduced emergency hospital admissions in seven major chronic disease populations, some of whom are considered at higher risk for COVID-19 morbidity and mortality.
Most of the medications are used in long-term community-based management for chronic diseases. Mean follow-up periods ranged from 9 to 45 months and most of the reported outcomes were hospitalisations for exacerbations or complications of the disease being treated (e.g., hospitalisation for heart failure in patients with chronic heart failure; hospitalisation for kidney disease in patients with type 2 diabetes).
Two treatments were for patients in emergency care settings (i.e., anticholinergics and early use of inhaled corticosteroids for acute asthma exacerbations presenting to the ED).
The number needed to treat to avoid one hospitalisation ranged from 5 to 115, with half of the reported treatment estimates reporting a number needed to treat less than 25.
Detailed evidence summaries for each medication and patient population are located below.
Chronic heart failure with reduced ejection fraction or left ventricular dysfunction
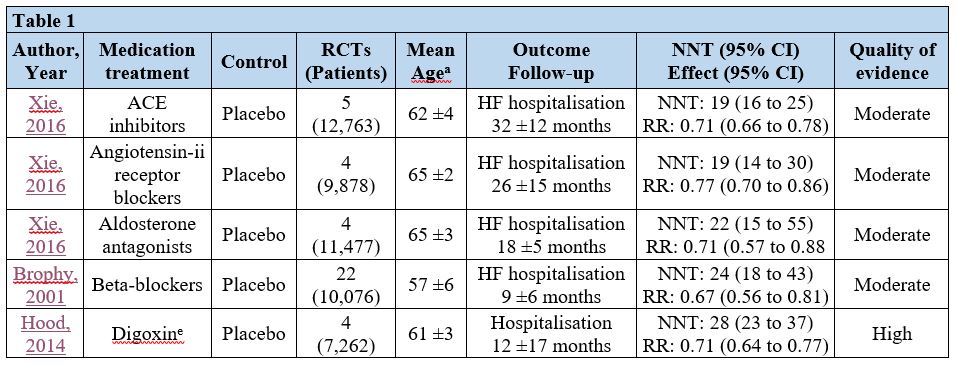 aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. dAnother meta-analysis (Le 2016) showed similar results. eFor patients in sinus rhythm. Abbreviations: ACE= angiotensin-converting enzyme; CI= confidence interval; HF= heart failure; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; RR= risk ratio.
aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. dAnother meta-analysis (Le 2016) showed similar results. eFor patients in sinus rhythm. Abbreviations: ACE= angiotensin-converting enzyme; CI= confidence interval; HF= heart failure; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; RR= risk ratio.
Stable coronary artery disease
 aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. Abbreviations: CI= confidence interval; HF= heart failure; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; RR= risk ratio.
aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. Abbreviations: CI= confidence interval; HF= heart failure; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; RR= risk ratio.
Hypertension
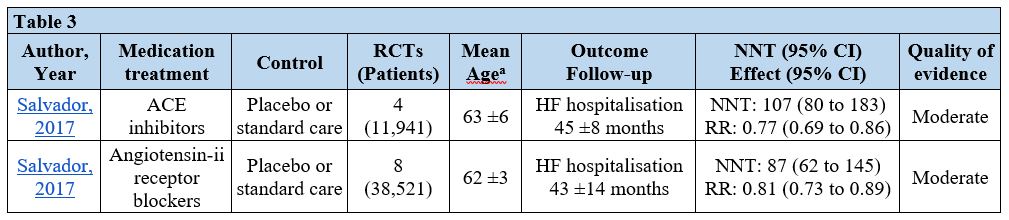 aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. Abbreviations: ACE= angiotensin-converting enzyme; CI= confidence interval; HF= heart failure; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; RR= risk ratio.
aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. Abbreviations: ACE= angiotensin-converting enzyme; CI= confidence interval; HF= heart failure; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; RR= risk ratio.
Type 2 diabetes
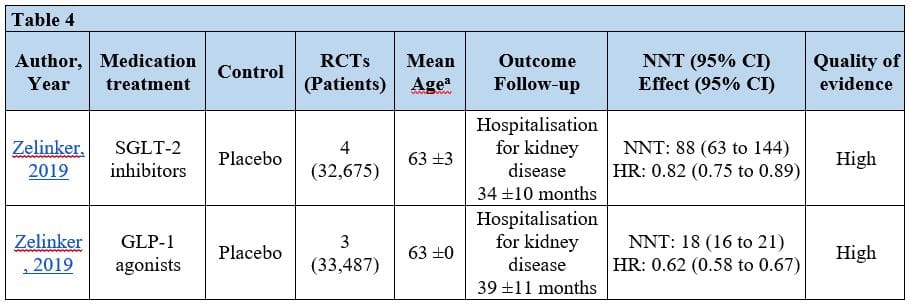 aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. Abbreviations: CI= confidence interval; GLP-1= glucagon-like peptide-1 receptor agonist; HF= heart failure; HR=hazard ratio; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; SGLT-2 = sodium-glucose transport protein 2 inhibitor.
aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. Abbreviations: CI= confidence interval; GLP-1= glucagon-like peptide-1 receptor agonist; HF= heart failure; HR=hazard ratio; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; SGLT-2 = sodium-glucose transport protein 2 inhibitor.
Chronic obstructive pulmonary disease (stable, moderate to severe)
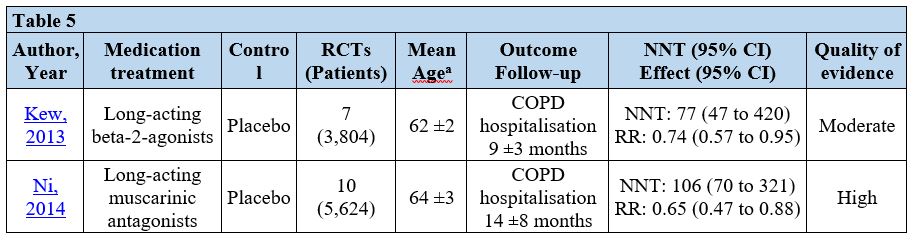 aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. Abbreviations: CI= confidence interval; COPD= chronic obstructive pulmonary disease; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; RR= risk ratio;.
aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. Abbreviations: CI= confidence interval; COPD= chronic obstructive pulmonary disease; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; RR= risk ratio;.
Acute asthma exacerbations in the emergency department
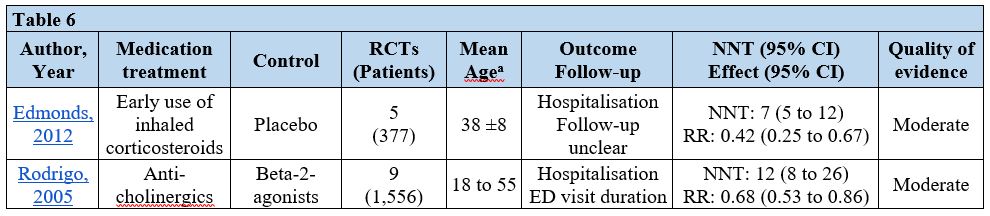 aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. Abbreviations: CI= confidence interval; ED= emergency department; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; RR= risk ratio.
aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. Abbreviations: CI= confidence interval; ED= emergency department; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; RR= risk ratio.
Schizophrenia
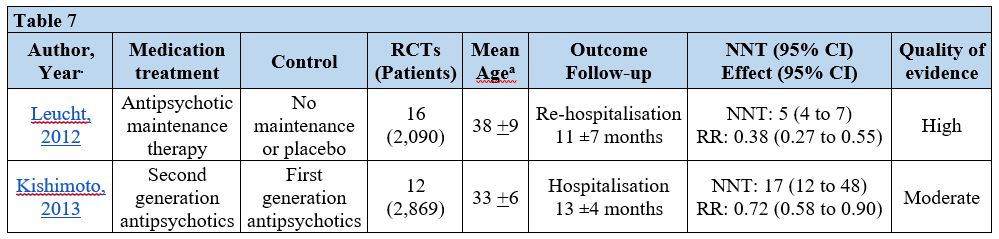 aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. Abbreviations: CI= confidence interval; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; RR= risk ratio.
aMean and standard deviation. Mean of means and median ages in trials contributing to the pooled estimate. bMean length of follow-up across trials. Mean of means, medians, and total study durations reported in trials contributing to the pooled estimate. cGrading of Recommendations Assessment, Development and Evaluation working group criteria. Abbreviations: CI= confidence interval; NNT= number needed to treat to avoid one emergency hospital admission; RCTs= randomised controlled trials; RR= risk ratio.
OUTCOMES OTHER THAN HOSPITAL ADMISSIONS
Our overview did not report outcomes other than hospitalisation. However, these medications have all been judged to have an acceptable balance of benefit to harm for these clinical indications by NICE guideline committees, which include patients, practitioners, managers, economists, policy-makers, NHS England, the Care Quality Commission, Public Health England, NHS Improvement, and Health Education England.
SPECIFIC MEDICATION SAFETY EVIDENCE AND GUIDANCE DURING THE COVID-19 PANDEMIC
We found COVID-19-related evidence and guidance on the safety of eight of the medications in our overview.
Angiotensin-converting enzyme (ACE) inhibitors, Angiotensin-ii receptor blockers (ARBs)
As of 1 May 2020, physician colleges and professional cardiology and hypertensive societies in Europe and North America recommend that ACE-inhibitors and ARBs should be continued among patients for whom treatment is indicated, including patients with hypertension and heart failure. However, if patients become infected with COVID-19 then dose adjustments may be considered to manage hypotension from dehydration and haemodynamic deterioration (American Heart Association, Heart Failure Society of America, American College of Cardiology,British and Irish Hypertensive Society, UK Royal College of Physicians, European Society for Cardiology).
The Royal College of General Practitioners has recommended that blood monitoring for patients on ACE-inhibitors is maintained by GPs to protect against electrolyte imbalances and kidney disease.
There has been speculation that ACE-inhibitors and ARBs may increase the severity of COVID-19 infection (Vaduganathan, Aronson, Rico-Mesa) and, therefore, should be stopped preemptively.
Current observational evidence involving COVID-19 patients does not support these hypotheses (Li 2020, Zhang 2020, Liu 2020, Yang 2020, Bean 2020). In fact, a growing number of observational studies have shown potential benefit in the form of reduced illness severity and mortality among patients taking ACE-inhibitors and ARBs. However, these studies are not randomised and should be interpreted with caution. Clinical trials assessing the impact of ACE-inhibitors and ARBs on outcomes in patients with COVID-19 are ongoing (NCT04329195, NCT04338009).
Statins
As of 1 May 2020, the National Institutes of Health and European Society for Cardiology recommend that statin therapy in coronary artery disease should generally be maintained regardless of COVID-19 status. However, the European Society for Cardiology suggests that temporary withdrawal may be appropriate if a patient develops severe rhabdomyolysis or increased liver enzymes in hospital. Other professional clinical organisations and societies have not published clear recommendations on alterations to statin therapy during the pandemic.
There is mixed evidence regarding the impact of statins on risk and severity of COVID-19 infection. A case series study from Wuhan published in March showed that COVID-19 patients had low levels of serum cholesterol. This prompted speculation that cholesterol lowering drugs may be associated with a higher risk of COVID-19 infection and worse outcomes (Ravnskov 2020). However, there are multiple observational cohort studies and at least one randomised clinical trial showing that statin therapy is associated with favourable outcomes in patients admitted to hospital with influenza or pneumonia (Virani 2020, European Society for Cardiology 2020) and, therefore, may serve a protective role once infected.
There are ongoing clinical trials examining the impact of statins on severity of COVID-19 infection (Ruxo-Sim-20, C-19-ACS, CRASH-19). In the meantime, the European Society of Cardiology COVID-19 guidelines do not suggest stopping, delaying or witholding statins.
Inhaled corticosteroids
As of 1 May 2020, clinical respiratory societies, guideline organisations, and medical research institutes have recommended that patients with asthma that routinely use inhaled corticosteroids for control of airway inflammation should continue using the medication in the community during the COVID-19 pandemic, and to follow their pre-established personal asthma action plan. (American Academy of Allergy Asthma and Immunology, United States National Institutes of Health, England’s National Institute for Health and Clinical Excellence, British Thoracic Society)
There is currently no evidence that use of inhaled corticosteroids increases the risk of getting COVID-19.
There is some debate about the use of systemic steroids among patients hospitalised with COVID-19. There are ongoing trials examining the protective role of inhaled corticosteroids for patients hospitalised with respiratory disease (NCT04331054). This issue is beyond the scope of this review but readers may refer to a rapid review of evidence by the Centre for Evidence-Based Medicine and guidance from the United States National Institutes of Health
Long acting beta-2-agonists (LABA), Long acting muscarinic antagonists (LAMA)
As of 1 May 2020, the National Institute for Health and Care Excellence recommends that patients with COPD continue to use their LABA and LAMA nebulisers. They have provided reassurance that the aerosol comes from the fluid in the nebuliser chamber and will not carry virus particles from the patient.
Sodium glucose co-transporter 2 inhibitors
As of 1 May 2020, there has been limited guidance on alterations to diabetes medications for people with type 2 diabetes not affected by COVID-19. However, if people with type 2 diabetes are hospitalised with acute illness, COVID-19 or other, it is recommended that patient stop taking SGLT-2 inhibitors due to the risk of diabetic ketoacidosis, and only restart them once a healthcare practitioner has confirmed that blood ketone levels are normal and the condition has stabilised (Diabetes UK, European Medicines Agency).
There has been speculation about a link between diabetes, diabetes medications, and poor COVID-19 outcome (Bornstein 2020, Ceriello 2020). However, these hypotheses have not been studied in people affected by COVID-19. Studies investigating these potential associations are ongoing (NCT04324736).
Antipsychotics
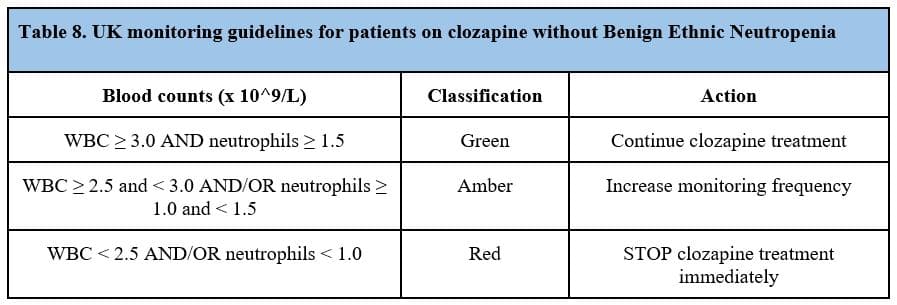
As of 1 May 2020, there is specific guidance on use of clozapine during the COVID-19 pandemic. The UK Royal College of Psychiatrists has re-published UK guidelines for monitoring white blood cell and neutrophil counts for patients on clozapine with specific thresholds for increasing monitoring and stopping therapy (Tables 8 and 9). These recommendations are based on trials and prospective cohort studies showing that clozapine use may result in neutropenia and agranulocytosis (Schulte 2006). The Royal College has suggested that these haematological side effects may increase the risk of COVID-19 infection and poor outcomes. However, the Royal College also emphasises the potential risk of discontinuing effective antipsychotic treatment at a time when uncontrolled psychotic symptoms may present challenges in safely managing COVID-19 infected patients. Therefore, they conclude that clozapine treatment should continue unless specific WBC and neutrophil thresholds are breached. This guidance has been echoed by an expert consensus statement on use of clozapine by the Treatment Response and Resistance in Psychosis working group. Similarly, the Royal College of General Practitioners has recommended that blood monitoring for patients on antipsychotics is maintained.

Narrative reviews and expert commentaries have suggested that antipsychotic medication, in general, may increase the risk of COVID-19 infection or exacerbate the severity of infection (Laporte 2020, Pandarakalam 2020). These claims are made based on observational studies showing that hospital admissions due to pneumonia are higher among clozapine treated patients (Abdelmawla 2009, Leung 2017, Stoecker 2017). Proposed mechanisms for the higher incidence of pneumonia-related hospitalisation are sialorrhea and aspiration, sedation, agranulocytosis, and a partial immuno-suppressant or immune-modulating effect. Currently, there is no direct evidence that antipsychotics increase risk of COVID-19 or worsen its severity.
GUIDANCE ON OPTIMISING USE OF HIGH-VALUE MEDICATIONS DURING THE COVID-19 PANDEMIC
Clinicians and researchers (Alexander 2020,Greenhalgh 2020) have provided recommendations for optimising medication use across all patient groups during COVID-19. These recommendations include:
- prevent stockpiling and drug shortages by restrict dispensing to 30 day intervals
- utilizing mail order and home delivery services for medication
- increasing the funding and scope of home delivery services
- relaxing refill criteria for high-priority medications to limit the need for medication review in patients with a history of stable disease on their current medication regimen
- remote consultations for medication review
- developing an essential medicines strategy in which are medicines that satisfy the priority health needs of the population be available in the health system at all times, in adequate amounts, and at an affordable price. This may take different forms in different health systems but the core concept is reducing barriers to access of high priority medications (no dispensing fee, adequate supply)
- explore longer term strategies to safeguard access including establishing and maintaining central inventories of essential medicines and increase domestic production of essential medicines
The are also clinical guidance documents with recommendations on optimising use of medications in some of the specific patient groups that we identified in our review.
The Royal College of General Practitioners has suggested that GPs prioritize ongoing management, including medication optimisation, for patients with chronic obstructive pulmonary disease (COPD), asthma, type 2-diabetes, and significant mental health concerns. They suggest that practitioners do the following:
- conduct remote medication reviews unless there are overriding reasons that a face-to-face assessment is necessary
- consider batch prescribingg. 6-12 months repeat prescribing of 28 day supplies to prevent supply issues
- avoid lengthening the duration of supplies of repeat medication unless clinically indicated
- dispense medications if a dispensing practice
The National Institute for Health and Care Excellence has provided the following recommendations to practitioners for optimising medications in patients with COPD and asthma during the pandemic:
- utilise remote consultations (and issue electronic prescriptions rather than paper)
- consider pharmacy deliveries, postal services, NHS Volunteer Responders or introducing drive-through pick-up points for medicines
- prescribe in 30-day intervals to protect the supply chain
CONCLUSIONS
During the current pandemic, it is critical that community-based patient treatments are optimised to limit unplanned hospital admissions. We identified 14 evidence-based, guideline-supported medications could be optimised to reduce hospital admissions: angiotensin-converting enzyme inhibitors, angiotensin-ii receptor blockers, aldosterone antagonists, beta-blockers, digoxin, statins, anticholinergics, inhaled corticosteroids, long-acting beta-2-agonists, long-acting muscarinic antagonists, sodium-glucose transport protein 2 inhibitors, glucagon-like peptide-1 receptor agonists, depot antipsychotic therapy, and second generation antipsychotics.
Implementing these treatments and seeing their benefits typically requires long follow-ups, patient engagement and ongoing clinical management. During pandemic lockdown, novel strategies are needed to support optimised use of the medications including telephone triage, video consultations, home delivery services, and prescribing practices (30 day refills) that aim to protect the supply chain. There may be value in generating evidence for interventions that may improve adherence to medication during lockdown.
With regards to medication safety, practitioners should continue to closely monitor WBC and neutrophils in patients taking clozapine. For patients with suspected or confirmed COVID-19 there are recommendations for considering dose adjustments (ACE-inhibitors, angiotensin-ii receptor blockers, antipsychotics) and stoppage (SGLT-2 inhibitors and antipsychotics) of some of the medications we identified. Practitioners should stay aware of ongoing clinical trials attempting to clarify the role of ACE-inhibitors, angiotensin-ii receptor blockers, statins, and inhaled corticosteroids in patients with confirmed COVID-19.
Disclaimer: the article has not been peer-reviewed; it should not replace individual clinical judgement and the sources cited should be checked. The views expressed in this commentary represent the views of the authors and not necessarily those of the host institution, the NHS, the NIHR, the Department of Health and Social Care, Massey College, or the University of Toronto. The views are not a substitute for professional medical advice.
AUTHORS
Niklas Bobrovitz BHSc, MSc, DPhil, is a Fellow at Massey College and a Medical Student at the University of Toronto.
Kamal R. Mahtani BSc, PhD, MBBS, PGDip, FRCGP is a GP, Associate Professor and Co-Director of the Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences.
Joseph J. Lee MRCGP, is a General Practitioner and doctoral researcher based at the Nuffield Department of Primary Care Health Sciences, University of Oxford
SEARCH TERMS AND DETAILS
Search for rapid overview update: 2016 to 2020
| PubMed |
| 1 |
((((((((admission[Title/Abstract]) OR admitted[Title/Abstract]) OR readmission[Title/Abstract]) OR re-admission[Title/Abstract]) OR readmitted[Title/Abstract]) OR re-admitted[Title/Abstract]) OR hospitali*[Title/Abstract]) OR rehospitali*[Title/Abstract]) OR re-hospitali*[Title/Abstract] |
| 2 |
Limited using built in Systematic Reviews filter |
| 3 |
Limited to adults (age 19+) |
Search for original systematic overview: database inception to 2016
| Medline |
| 1 |
Hospitalization/ |
| 2 |
Patient admission/ |
| 3 |
Patient readmission/ |
| 4 |
(admission? or admitted or readmission? or re-admission? or re admitted or readmitted or hospitali* or rehospitali* or re-hospitali*).ti,ab. |
| 5 |
1 or 2 or 3 or 4 |
| 6 |
Cochrane database of systematic reviews.jn. or search.tw. or meta-analysis.pt. or Medline.tw. or systematic review.tw. |
| 7 |
5 and 6 |
| Cochrane Database of Systematic Reviews |
| 1 |
MeSH: Hospitalization |
| 2 |
MeSH: Patient Admission |
| 3 |
(admission or admitted or readmission or re-admission or re admitted or readmitted or hospitali* or rehospitali* or re-hospitali*):ti,ab |
| 4 |
(#1 OR #2 OR #3) |
| Database of Abstracts of Reviews of Effects |
| 1 |
MeSH: Hospitalization |
| 2 |
MeSH: Patient Admission |
| 3 |
(admission or admitted or readmission or re-admission or re admitted or readmitted or hospitali* or rehospitali* or re-hospitali*):ti,ab |
| 4 |
(#1 OR #2 OR #3) |
| PubMed |
| 1 |
((((((((admission[Title/Abstract]) OR admitted[Title/Abstract]) OR readmission[Title/Abstract]) OR re-admission[Title/Abstract]) OR readmitted[Title/Abstract]) OR re-admitted[Title/Abstract]) OR hospitali*[Title/Abstract]) OR rehospitali*[Title/Abstract]) OR re-hospitali*[Title/Abstract] |
| 2 |
Date limited to six months before search date (to capture articles not yet indexed in MEDLINE) |
| 3 |
Limited using built in Systematic Reviews |
| Grey literature |
| Google scholar targeted search |
| 1 |
(((hospital* OR (hospital AND admi*) OR (redmi*) OR (redmi*)) AND ((systematic review) OR (literature review) OR ((meta) AND (analy*))) AND ((random*) OR (trial) OR (RCT))) |
| 2 |
Sorted by relevance |
| Google scholar broad search |
| 1 |
Hospital admissions AND interventions AND systematic review |
| 2 |
Sorted by relevance |
| National Institutes of Health Research Website
https://www.journalslibrary.nihr.ac.uk/programmes/
Journals library; ongoing research; programme studies, all statuses; health technology assessment programmes |
| 1 |
hospital admissions |
| Research Council United Kingdom Website (seven major funding agencies)
http://gtr.rcuk.ac.uk/search/publication?term=admission+AND+systematic+review&fetchSize
=25&selectedSortableField=score&selectedSortOrder=DESC&fields=per.on%2Cper.fn%
2Cpub.a%2Cper.sn%2Cper.org.n%2Cpub.t%2Cper.pro.abs%2Cper.pro.t%2Cper.fnsn
%2Cpro.t%2Corg.n%2Cpro.gr%2Cpro.a |
| 1 |
Hospital admissions (journal article/review) |
| 1 |
Admission AND systematic review |
| 1 |
Admission AND review |
| King’s Fund Website http://kingsfund.koha-ptfs.eu |
| 1 |
Unplanned hospital admissions |
| 2 |
Unscheduled hospital admissions |
| 3 |
Emergency hospital admissions |
| 4 |
1 OR 2 OR 3 |
| 5 |
Review |
| 6 |
4 AND 5 |
Search for emerging COVID-19 clinical evidence and guidance on health care delivery
We included emerging evidence on the safety of the medications we identified and guidance for optimising use of the medications in the context of the COVID-19 pandemic (i.e., medication prescribing, dispensing, delivery, and adherence).
We screened all COVID-19 articles published in April and May 2020 by five high impact journals and 32 of their associated journals; JAMA network (94 articles screened), BMJ (109 articles screened), Lancet network (97 articles screened), New England Journal of Medicine (72 articles screened), and Annals of Internal Medicine (29 articles screened).
We searched for the most updated COVID-19 health care policy and guidance documents released by NICE, Royal College of Physicians, Royal College of General Practitioners, and the National Health Service.
We conducted 14 Google searches using synonyms for each of the included 14 medications and synonyms for COVID-19 (i.e., novel coronavirus, sars cov 2). We screened the first 20 hits for each search.
REFERENCES
Bobrovitz, N. (2019). Identifying and prioritising interventions to reduce emergency hospital admissions [PhD thesis]. University of Oxford.
Bobrovitz N, Heneghan C, Onakpoya I, et al. Medications that reduce emergency hospital admissions: an overview of systematic reviews and prioritisation of treatments. BMC Med. 2018;16(115). doi:10.1186/s12916-018-1104-9