Preventing respiratory illness in older adults aged 60 years and above living in long-term care
March 28, 2020
Patricia Rios, Amruta Radhakrishnan, Sonia M. Thomas, Nazia Darvesh, Sharon E. Straus, Andrea C. Tricco
This work was supported through the Canadian Institutes of Health Research (CIHR) through the Strategy for Patient Oriented-Research (SPOR) Evidence Alliance and commissioned by the Infection Prevention & Control, Health Emergency Programme, World Health Organization. We have prepared a summary of our report on behalf of the Oxford COVID-19 Evidence Service Team
Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences,
University of Oxford
Li Ka Shing Research Institute, Knowledge Translation Program, St. Michael’s Hospital
Correspondence to Andrea.Tricco@unityhealth.to
VERDICT
Overall, the results of the included systematic reviews suggest that high quality evidence supports treating residents with antiviral chemoprophylaxis with adamantine, as well as adamantine in combination with personal protective equipment. For the rest of the strategies, there was either no evidence of effectiveness (e.g., social isolation) or mixed evidence of effectiveness (e.g., rimantadine, zanamivir, hand hygiene, personal protective equipment). The mixed evidence on hand hygiene and use of personal protective equipment does not imply these should not be used in outbreaks
BACKGROUND
The Infection Prevention & Control of the World Health Organization (WHO) Health Emergency Programme commissioned a review on preventing and managing COVID-19 in older adults aged 60 years and above living in long-term care facilities. The overall objective of this rapid overview of reviews (overview hereafter) was to identify evidence on infection protection and control measures for adults aged 60 years and older in long-term care settings from systematic reviews. In order to focus the research question to increase feasibility, we proposed the following key research questions:
1. What are the infection prevention and control practices/measures for preventing or reducing respiratory viruses (including coronavirus and influenza) in older adults aged 60 years and above living in long-term care?
2. How do infection prevention and control practices differ for adults aged 60 years and above living in long-term care with respiratory illness and severe comorbidities or frailty differ than those without such severe comorbidities/frailty?
3. How do infection prevention and control practices differ for adults aged 60 years and above living in long-term care with respiratory illness from low- and middle-income economy countries (LMIC) differ than those living in high-income economy countries and do differences exist across different cultural contexts?
CURRENT EVIDENCE
Preventing respiratory illness in long-term care facilities:
One high quality SR3 found mixed results for the effectiveness of hand hygiene to prevent infection with 2 studies reporting statistically significant positive results in favour of hand hygiene and 1 study reporting non-statistically significant results. One moderate quality SR5 with meta-analysis found a moderate non-statistically significant effect in favour of personal protective equipment (PPE) in preventing infection. The same SR5 and meta-analysis also examined the effectiveness of social isolation to prevent infection and found no statistically significant results. One moderate quality SR5 reported statically significant evidence for the effectiveness of amantadine and amantadine + PPE to prevent the spread of viral respiratory infections in long-term care facilities.
Managing respiratory illness in long-term care facilities:
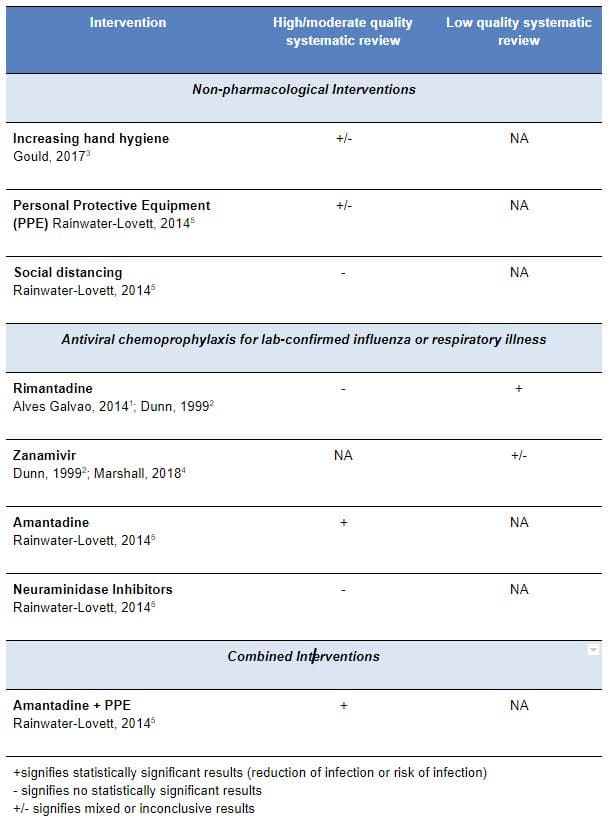
Statistically significant results were found from one moderate quality systematic review5 for the use of amantadine as antiviral chemoprophylaxis for individuals diagnosed with lab-confirmed influenza (Table 1). In addition, statistically significant results were found from one moderate quality systematic review for the use of amantadine plus personal protective equipment to prevent spread of infection from individuals diagnosed with lab-confirmed influenza. Statistically significant results were not observed in one moderate5 and one high1 quality systematic review regarding rimantadine or neuraminidase inhibitors as antiviral chemoprophylaxis. However, statistically significant results were observed in one low quality systematic review2 for rimantadine as antiviral chemoprophylaxis. Mixed evidence was identified from two low quality systematic reviews2,4 for zanamivir as antiviral chemoprophylaxis that reported non-statistically significant reductions in viral respiratory infection rates.
Table 1: Summary of evidence for included systematic reviews
EMERGING EVIDENCE IN COVID-19
None applicable
CONCLUSIONS
● The results suggest that high quality evidence supports treating residents with antiviral chemoprophylaxis with adamantine, as well as adamantine in combination with personal protective equipment (PPE)
● There was either no evidence of effectiveness (e.g., social isolation) or mixed evidence of effectiveness (e.g., rimantadine, zanamivir, hand hygiene, personal protective equipment) for other strategies examined in the included reviews
● However, the mixed evidence on hand hygiene and use of PPE does not imply they should not be employed during an outbreak
medrxiv.rog pre-print link: https://www.medrxiv.org/content/10.1101/2020.03.19.20039081v1
End.
Disclaimer: the article has not been peer-reviewed; it should not replace individual clinical judgement and the sources cited should be checked. The views expressed in this commentary represent the views of the authors and not necessarily those of the host institution, the NHS, the NIHR, or the Department of Health and social Care. The views are not a substitute for professional medical advice.
SEARCH TERMS
Comprehensive literature searches addressing all research questions were developed by an experienced librarian for MEDLINE, EMBASE, the Cochrane Library, and biorxiv.org/medrxiv.org databases. Grey (i.e., difficult to locate or unpublished) literature was located using keyword searches of relevant terms (e.g. respiratory illness, MERS, coronavirus, SARS, long-term care facilities) in clinicaltrials.gov and GIDEON (Global Infectious Diseases and Epidemiology Network).
Funding Statement: This work was funded by the Canadian Institutes of Health Research (CIHR) through the Strategy for Patient Oriented-Research (SPOR) Evidence Alliance
REFERENCES
1. Alves Galvão MG, Rocha Crispino Santos MA, Alves da Cunha AJ. Amantadine and rimantadine for influenza A in children and the elderly. Cochrane Database Syst Rev. 2014 Nov 21;(11):CD002745.
2. Dunn CJ, Goa KL. Zanamivir: a review of its use in influenza. Drugs. 1999 Oct;58(4):761-84. Review.
3. Gould DJ, Moralejo D, Drey N, Chudleigh JH, Taljaard M. Interventions to improve hand hygiene compliance in patient care. Cochrane Database Syst Rev. 2017 Sep 1;9:CD005186. doi: 10.1002/14651858.CD005186.pub4. Review.
4. Marshall L, Stevens G, Cordaro C. Managing influenza outbreaks in long-term care facilities. Consultant Pharmacist. 2018; 33(10):580.
5. Rainwater-Lovett K, Chun K, Lessler J. Influenza outbreak control practices and the effectiveness of interventions in long-term care facilities: a systematic review. Influenza Other Respir Viruses. 2014 Jan;8(1):74-82. doi:10.1111/irv.12203. Epub 2013 Nov 7. Review.
6. Volkman JC, Rebmann T, Hilley S, Alexander S, Russell B, Wagner W. Infection prevention disaster preparedness planning for long-term care facilities. Am J Infect Control. 2012 Apr;40(3):206-10. doi: 10.1016/j.ajic.2011.03.029. Epub 2011 Aug 15.