Risks of and from SARS-COV-2 (COVID-19) infection in people with asthma
March 1, 2021
Jamie Hartmann-Boyce (corresponding author), DPhil, Nuffield Department of Primary Care Health Sciences, University of Oxford, UK. Jamie.hartmann-boyce@phc.ox.ac.uk; 01865 289 206. Radcliffe Primary Care Building, Radcliffe Observatory Quarter, Woodstock Road, Oxford, UK, OX2 6GG.
Karen Rees, PhD. Freelance systematic reviewer, Warwick, UK.
Afolarin Otunla, BA, Medical Sciences Division, University of Oxford, Oxford, Oxfordshire, UK
Jana Suklan, PhD, NIHR Newcastle In Vitro Diagnostics Co-operative, Newcastle University, Newcastle, United Kingdom
Ella Schofield, Medical Sciences Division, University of Oxford, UK.
James Gunnell, Medical Sciences Division, University of Oxford, UK.
Alexandra Mighiu, DPhil, Medical Sciences Division, University of Oxford, UK.
Richard Hobbs, FMedSci, Nuffield Department of Primary Care Health Sciences, University of Oxford, UK.
Paddy Dennison, PhD, MRCP, University Hospitals Southampton NHS Foundation Trust, Southampton, UK.
Acknowledgements: WHO commissioned and financially supported this work. JS is supported by the NIHR Newcastle In Vitro Diagnostics Co-operative. The views expressed are those of the author and not necessarily those of the NIHR, the NHS or the Department of Health and Social Care.
Pdf to Download
Background
In the context of the COVID-19 pandemic, WHO and WHO Member States are requesting information and guidance on key topics related to COVID-19 and the virus which causes the disease SARS-COV-2. This rapid review was commissioned to address specific key questions for WHO to provide high-quality, evidence-informed information products around COVID-19.
This review presents a summary of the latest research evidence on the effects of COVID-19 in people with asthma (PWA).
At the outset of the pandemic, PWA were assumed to be at increased risk from COVID-19. However, as data emerged throughout 2020 the association between asthma and COVID-19 appeared less clear than initially assumed, with some studies suggesting excess risk and other suggesting no excess risk, or in some cases, diminished risk.(1) It is important to establish the relationship between asthma and COVID-19-related outcomes in order to provide effective guidance to PWA, their carers, healthcare providers, and policymakers.
Therefore, in this rapid review, we set out to review the evidence regarding whether PWA are at increased risk of infection with the virus that causes COVID-19, and/or of suffering complications or death. In particular, we set out to analyse evidence on the following questions:
- Is asthma associated with increased risk of acquiring COVID-19?
- Is asthma associated with hospitalization with COVID-19?
- Is asthma associated with the severity of COVID-19 outcomes?
Methods
A protocol was agreed in advance with the WHO, and methods follow a general framework for a suite of rapid reviews commissioned by WHO in respect to their scientific briefs on COVID-19 and selected non-communicable diseases.(2) This follows a four-stage process, set out below.
(1) Searches
We searched the Cochrane COVID-19 study register, Embase, MEDLINE, and LitCOVID on 8 October 2020 for published literature or literature accepted for publication but not yet published, in any language (see Appendix 1 for MEDLINE and EMBASE strategies). Two reviewers screened titles and abstracts, and full texts of selected references, with discrepancies resolved by discussion or referral to a third reviewer. We selected studies according to the following inclusion criteria:
- Population: people diagnosed with asthma, with no limitations by age, disease severity, or duration.
- Exposure: SARS-COV-2 infection
- Comparator: people without asthma
- Outcome: Rates of COVID-19: confirmed infection; hospitalisation; admission to ICU; death. Where reported, we also extracted information on the specified outcomes where broken down by asthma medication, age, ethnicity, BMI, and co-morbidities.
- Study types: Systematic reviews (see stage 2), with a very broad definition as articles which systematically searched at least one database; and primary studies (see stage 3), including prospective and retrospective cohort studies and case-control studies, but excluding case reports and case series
(2) Review relevant systematic reviews
Two reviewers next appraised and extracted data from systematic reviews in relation to the above review questions, with discrepancies resolved by discussion. We included any systematic reviews which met the above criteria. Quality was assessed using a modified version of the AMSTAR-2 checklist, focussing only on critical domains, namely: protocol registered before commencement; adequacy of literature search; justification for excluding individual studies; risk of bias from individual studies; appropriateness of meta-analytical methods; consideration of risk of bias when interpreting results; assessment of presence and likely impact of publication bias.(3) Appraisal was not used as a basis for excluding reviews but was used when considering certainty in the findings from said reviews. Data from contributing systematic reviews were narratively synthesised.
As pre-specified with the WHO, we used our assessments of the systematic review literature to determine whether primary literature also needed to be included in the scientific briefing and rapid review (i.e. due to inadequacies in existing systematic reviews). We judged this to be the case and hence moved on to stage 3 (see below).
(3) Review relevant primary studies
Given gaps in the systematic review literature, we went on to review and extract data from primary studies. Two reviewers extracted data and appraised quality using the Newcastle Ottawa Scale for observational studies; again, discrepancies were resolved by discussion or referral to a third reviewer.
(4) Findings and key characteristics of these studies are summarised.
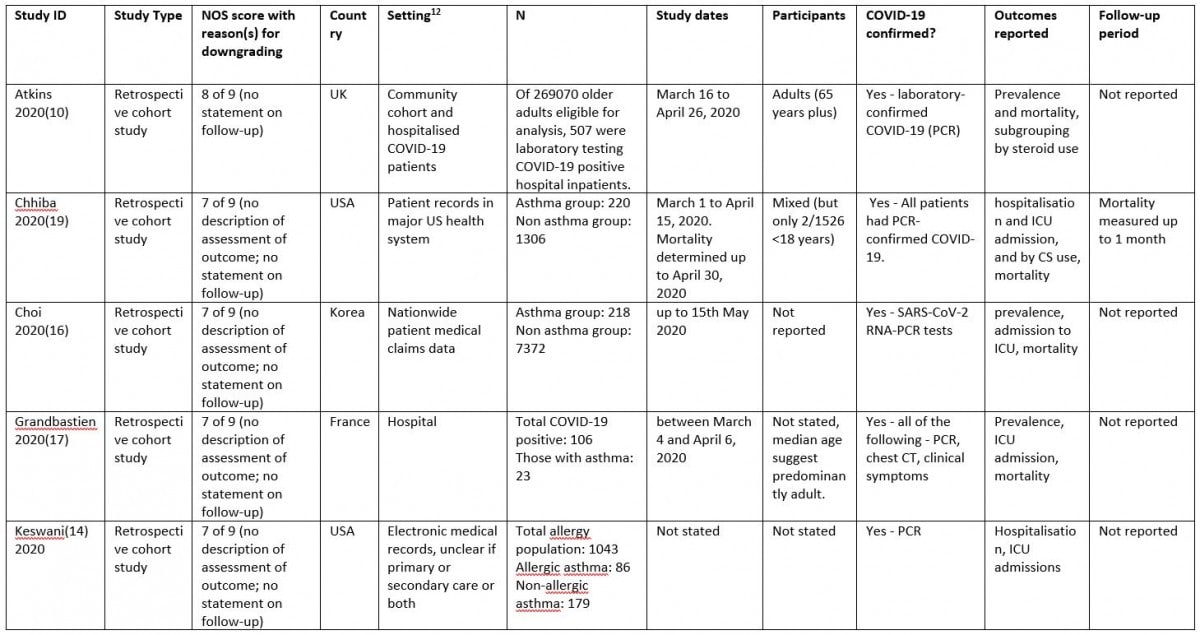
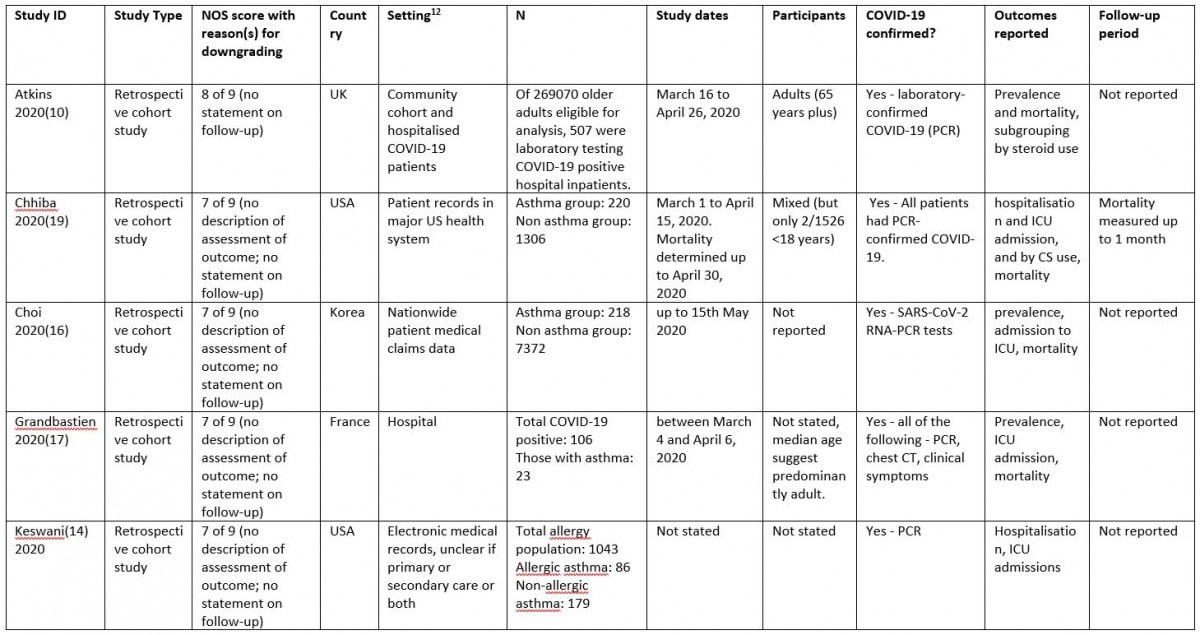
As specified in advance, only studies judged to be at low risk of bias were incorporated in the narrative synthesis. For the purposes of this review, we judged low risk of bias to be an NOS score >6 (out of 9).
Results
Search results
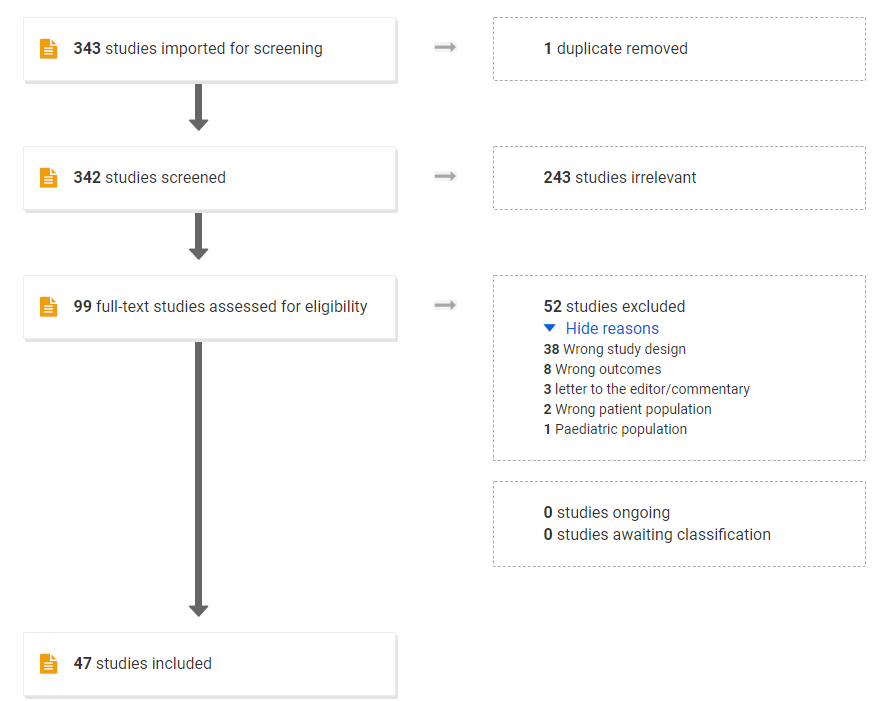
After removing duplicates, our searches returned 342 references. Six systematic reviews and 41 primary studies met our PICO criteria; after assessing quality, 13 of these primary studies met criteria for feeding into our work with WHO. The most common reason for exclusion at full-text stage was ‘wrong study design’ (see Figure 1).
Characteristics of included reviews
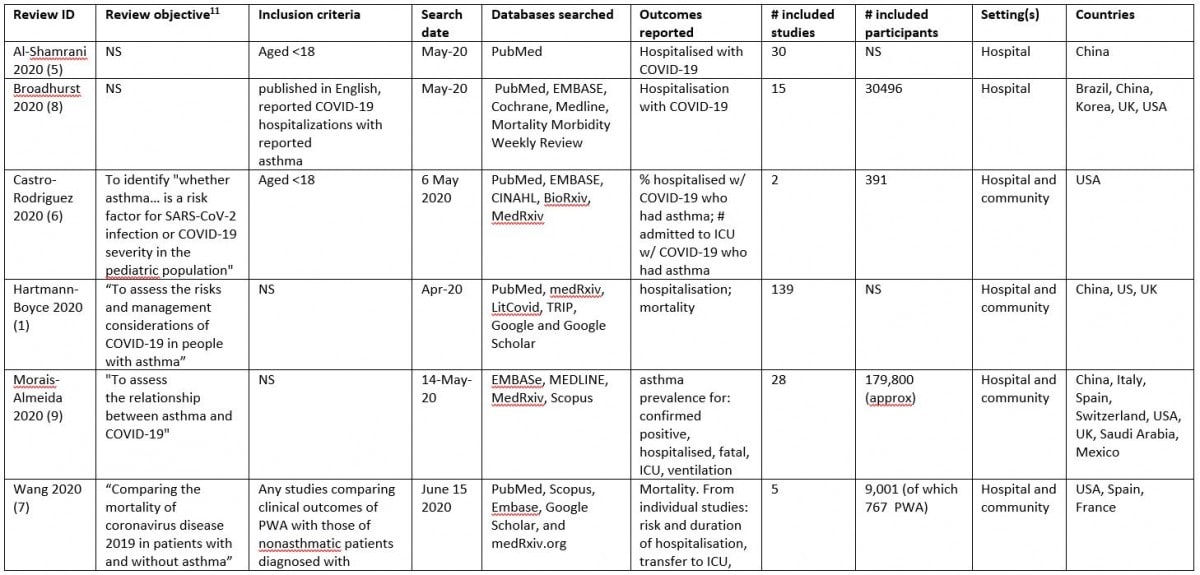
We found six systematic reviews which addressed at least one of our research questions. As our definition of ‘systematic review’ was less rigid than would be used in other contexts, given the paucity of research in this area, all were included. None of the authors declared relevant funding or conflicts of interest. Of the included reviews, the most recent search date was June 2020 (Supplemental Table 1).
Two reviews (Al-Shamrani 2020 and Castro-Rodriguez 2020) focussed on a range of COVID-19 outcomes in paediatric populations.(5, 6) Two reviews focussed on specific outcomes: Wang 2020 evaluated COVID-19 mortality in adults with asthma (7) and Broadhurst 2020 evaluated COVID-19 hospitalisations in adults with asthma.(8) The final two reviews were broad in nature: Hartmann-Boyce 2020 was a rapid review focussing on risks and management considerations relating to COVID-19 and asthma(1), and Morais-Almeda 2020 reviewed literature covering a broad spectrum of topics related to asthma and COVID-19.(9) Key characteristics from the included systematic reviews can be found in Supplemental Table 1. As seen in Supplemental Table 2, with the exception of Wang 2020 (7), which had no critical weaknesses, all included reviews were judged to have at least four critical weaknesses by AMSTAR-2 criteria.
As only Wang 2020 was judged to be free of critical weaknesses, and as Wang 2020 only evaluated mortality outcomes, did not find a definitive answer due to lack of data, and last searched for literature in June 2020 (which given the pace of COVID-19 research risks being out of date), we judged that there were considerable gaps in the systematic review literature regarding all of our research questions, which warranted taking into account key primary studies when preparing the WHO Scientific Brief.
Characteristics of primary studies
Twelve retrospective cohort studies and one prospective cohort study were judged to be of sufficient quality to be included in this synthesis (NOS ratings >6 of 9). Characteristics of these can be found in Supplemental Table 3; detail on studies identified which did not meet our threshold for inclusion in this synthesis can be found in Appendix 2. These studies may be incorporated in a subsequent synthesis, done outside of the WHO brief, and are included here for reference for interested readers.
Is asthma associated with increased risk of acquiring COVID-19 or with hospitalisation with COVID-19?
None of the included reviews were able to deduce with any certainty whether asthma was associated with increased risk of acquiring COVID-19. Hartmann-Boyce concluded that “As community testing for COVID-19 remains limited in many parts of the world, it is impossible to say with any certainty if any groups are more or less likely to contract the disease.”(1) For this reason, most of the data on prevalence comes from hospitalised cohorts.
Of the reviews in paediatric populations, Al-Shamrani concluded that children with asthma do not have a higher risk of infection with COVID-19. However, reflecting a paucity of data on COVID-19 in paediatric populations, their conclusions were based on data from two Chinese studies in adults, both of which found a lower prevalence of asthma in COVID-19 cases than in the general population.(5) Castro-Rodriguez looked at data from two small studies which did not compare asthma rates to population prevalence: in the first, 40/345 children with COVID had “chronic lung diseases (including asthma)”; in the second, 11/46 children hospitalised with COVID-19 had asthma. These samples are too small to enable any conclusions to be drawn.(6)
Due to the nature of COVID-19 testing, particularly early in the pandemic, most studies which looked at COVID-19 prevalence were in hospitalised cohorts; two reviews reported data on asthma prevalence within this context. Broadhurst charted the proportion of PWA among patients hospitalised with COVID-19 against each study site’s asthma prevalence and found the proportions were similar across all studies, leading them to conclude that asthma prevalence among those hospitalized with COVID-19 appears similar to population asthma prevalence, and that this was significantly lower than asthma prevalence in those hospitalised for influenza, but caution that it is possible that reporting of comorbidities was done inconsistently across studies.(8) Morais-Almeida reported asthma prevalence in those hospitalised with COVID-19 ranging from 0.3 to 17.9% (median 8.6%) but did not formally compare this to asthma rates in the community.(9)
Four primary studies compared COVID-19 rates in PWA to those in people without asthma (Table 4). In three of the four, data suggested an increased infection rate in PWA than in people without asthma; in two of the four, this difference was statistically significant, though in one the lower bound of the confidence interval narrowly excluded no difference and the point estimate for association was modest (1.08).
There is no way to establish whether a possible increase in COVID-19 infections in PWA is due to a genuine increase in infection, or due to PWA being more likely to show symptoms of COVID-19 or be hospitalised with COVID-19. Together the latter are the predominant prompts for COVID-19 testing. Further data from community testing initiatives, including asymptomatic patients, are needed to adequately answer any question regarding infection rates.
Table 1. Estimates regarding prevalence of infection and/or risk of hospitalisation with COVID-19 in PWA
| Study ID[1] |
Setting |
Prevalence of asthma in people with COVID-19 |
Direction of association (double arrows represent statistical significance) |
| Atkins 2020(10) |
Community cohort and hospitalised COVID-19 patients |
COVID-19 positive: 90/507 – 17.6%
Rest of cohort (without COVID-19): 34612/268563 -12.9% |
↑ |
| Kim 2020(11) |
Hospital |
3.2% (similar to prevalence in the general population of Korea) |
↔ |
| Yang 2020(12) |
Data obtained from the Health Insurance Review & Assessment Service of Korea |
683 COVID-19 positive/29570 PWA – 2.3%
Adjusted for age and sex: OR 1.07 (1.0, 1.15)
Fully adjusted: OR 1.08 (1.01, 1.17) |
↑↑ |
| Zhu 2020(13) |
UK Biobank – hospitalised patients with severe COVID-19 |
Asthma overall: SARS-CoV-2 PCR test during hospitalisation, positive 116/65677 (0.18%)
Unadjusted: 1.44 (1.18, 1.76); Adjusted: 1.39 (1.13, 1.71) |
↑↑ |
A further two primary studies using data in Covid-19 positive patients, derived from electronic health records, estimated odds of hospitalisation with COVID-19 in PWA compared to people without asthma. Neither found statistically significant associations, but whether this is down to small samples or genuine lack of association is unclear (Keswani, non-allergic asthma OR 1.03 (95% CI 0.75 to 1.31), allergic asthma OR 0.77 (95% CI 0.57 to 1.03), Mahdavinia OR 1.08 (95% CI 0.77 to 1.53)).(14, 15)
Conclusion: data are insufficient to conclude whether or not asthma predisposes to infection or hospitalisation with COVID-19. There are some data from primary studies suggesting PWA may be over-represented in people hospitalised with COVID-19, but the two primary studies presenting adjusted odds ratios did not find a statistically significant association. Data is inconsistent across systematic reviews, and studies contributing data may be limited by inaccurate or differential recording of co-morbidities, in addition to limitations in populations tested. There is insufficient data on paediatric populations to draw any conclusions in this group.
Is asthma associated with severity of COVID-19 outcomes?
ICU admission
One review (Castro-Rodriguez) looked at risk of PICU admission with COVID-19 and found “scarcely any data.” In the one study they included that reported this outcome, of 46 children hospitalised with COVID-19, no differences in proportions admitted to general floor versus PICU (8 (asthma) /33 general, 3 (asthma)/13 PICU) were found.(6) One review (Morais-Almeda) evaluated ICU admission.(9) Of the five studies they included which reported data on this outcome, three had data on <200 participants. In one study with 200 hospitalised patients in Switzerland, the prevalence of asthma in those on mechanical ventilation was 2.7%. In 1000 hospitalised adult patients in the US, prevalence of asthma was 12.3% in those admitted to ICU. Neither of these figures clearly signal an increased risk of ICU admission in PWA with COVID-19, but no formal analyses were conducted. None of the five primary studies we included that tested for an association between asthma and admission to the ICU with COVID-19 detected a statistically significant one, but confidence intervals were wide in all analyses (Table 2).
Table 2. Estimates from primary studies on the association between asthma and risk of ICU admission with COVID-19
| First author/Year |
Estimates of risk of ICU admission in patients with asthma and
COVID-19, compared to people without asthma with COVID-19 |
Direction of association (double arrows represent statistical significance) |
| Choi 2020(16) |
asthma: 7/218 (3.2%); no asthma: 208/7372 (2.8%), P=0.73
univariate: OR 1.14 (0.53, 2.46), P=0.73
multivariate: OR 0.66 (0.3, 1.46) controlling for age, sex, comorbitity, P=0.3 |
↔ |
| Grandbastien 2020(17) |
Propensity score adjusted analysis; asthma not risk factor for transfer to the intensive care unit (OR, 1.065; 95% CI, 0.272-3.522;P=.92).[2] |
↔ |
| Kim 2020(11) |
Multivariate analysis Model 1: OR 1.02 (0.39, 2.66)
Multivariate analysis Model 2: OR 1.12 (0.35, 3.54)[3] |
↑ |
| Keswani 2020(14) |
Allergic asthma: OR 1.02 (0.69, 1.51); Non-allergic asthma: OR 1.31 (0.85, 1.99). Adjustment for age, sex, BMI, race |
↑ |
| Mahdavinia 2020(15) |
OR 1.18 (0.45, 1.32) (no further detail given) |
↑ |
Mortality
Two reviews looked at whether asthma was associated with death with COVID-19. Morais-Almeida looked at data across studies but did not synthesise these data. In the three studies included in Morais-Almeida with >200 participants that evaluated death, one found no association, one found PWA were under-represented in deaths from COVID-19, and one (OpenSAFELY) found a higher risk of COVID-19 hospital death in PWA (fully adjusted HR = 1.11; 95% 1.02–1.20), with a greater HR for those with recent use of an oral corticosteroid (OCS) (HR = 1.25; 95% CI 1.08–1.44). OpenSAFELY was the only one of these three studies identified as a high-quality primary study in our review and is a very large observational study based on routinely collected data.(18)
Wang conducted a meta-analysis with data from 4 studies, including 744 PWA and 8,151 people without asthma. They found no significant association between asthma and mortality with COVID-19 (OR = 0.96; 95% CI 0.70–1.30; I2 = 0%; p = 0.79). Results were stable in a sensitivity analysis. We did not judge this review to have any critical weaknesses.(7)
In addition to the OpenSAFELY estimates presented above, a further six primary studies we included evaluated associations between asthma and death with COVID-19. Of these, none detected a statistically significantly increased risk of death (Table 6). One detected a statistically significant reduced odds of death with COVID-19 in PWA.
Table 3. Estimates from primary studies on the association between asthma and risk of death with COVID-19
| First author/Year |
Estimates of risk of mortality in patients with asthma and
COVID-19, compared to people without asthma with COVID-19 |
Direction of association (double arrows indicate statistical significance) |
| Atkins 2020(10) |
Demographics model: OR 0.88 (0.51 to 1.50)[4]
Full model: OR 0.59 (0.33, 1.04)[5] |
↓ |
| Chhiba 2020(19) |
asthma: 8/220 (3.6%)
no asthma: 64/1306 (4.9%) |
↓ |
| Choi 2020(16) |
asthma: 17/218 (7.8%); no asthma: 210/7372 (2.8%), P<0.001
univariate: OR 2.89 (1.73, 4.8), P<0.001
multivariate: OR 1.32 (0.71, 2.5) controlling for age, sex, co-morbitity, P=0.39 |
↑ |
| Kim 2020(11) |
Multivariate analysis Model 1: OR 1.76 (0.81, 3.82)
Multivariate analysis Model 2: OR 1.66 (0.62, 4.4), P=0.31[6] |
↔ |
| Mahdavinia 2020(15) |
OR 2.56 (0.57, 11.5) (no detail given re: adjustment) |
↔ |
| Santos 2020(20) |
Univariate: HR 0.66 (95% CI 0.61, 0.73)
Multivariate: HR 0.71 (0.61, 0.81)[7] |
↓↓ |
| Williamson 2020(18) |
Fully adjusted: HR = 1.11; 95% 1.02–1.20 |
↑↑ |
Conclusion: data are insufficient to conclude whether or not asthma predisposes to ICU admission or death with COVID-19. Systematic reviews are inconclusive. The one meta-analysis conducted found no increased risk of mortality, but confidence intervals were wide. Primary studies have conflicting results, with no clear signal of direction of association across studies, although the largest observational study showed increased risk for PWA with recent need for OCS to control an exacerbation. An up to date meta-analysis is needed, taking into account the effect of adjusting for different confounders on the associations of interest.
Do COVID-19 outcomes in PWA differ based on population characteristics?
None of the included reviews evaluated whether outcomes differed based on the population characteristics specified in our protocol (age, ethnicity, BMI, asthma medication, asthma severity/type, co-morbidities).
Ten primary studies looked at least one of the above characteristics (beyond simply adjusting for them in their analyses). Data regarding our pre-specified characteristics reported in more than one study can be found in Table 7. Very few studies were sufficiently powered to detect a difference by subgroups within PWA. Data on ICS use were not consistent across studies, but the largest study of its type found high dose ICS was associated with higher risk of COVID-19 mortality when compared to SABA. A second study using the same data set found OCS use was also associated with greater risk in people with asthma; no other studies evaluated OCS use. Where associations were detected, it was unclear if these were due to mechanisms of the medications themselves, or due to the association between prescriptions for these medications and asthma severity. With the exception of the one study comparing ICS to SABA, no significant associations were found between SABA and LABA and disease outcomes. People with allergic asthma seem at lower risk of severe outcomes from COVID-19 than those with non-allergic asthma, but again more data are needed to confirm this. People with COPD and asthma appear at higher risk from severe COVID-19 outcomes than PWA who do not have COPD. In PWA, risk from COVID-19 increases with age, as in the general population.
Only one study reported on ethnicity.(21) Wang 2020 explicitly set out to look at risk factors for hospitalisation, intensive care, and mortality among patients with asthma and COVID-19. In univariate analyses using white ethnicity as a reference group, all other ethnic groups had higher risks of hospitalisation. The association was statistically significant for Black and Asian groups, and remained so in an age-stratified multivariate logistic regression. No statistically significant associations with ethnicity were found for ICU or death outcomes; this may reflect lower statistical power for these outcomes. Only one study looked at BMI. Kim 2020 found that the association between asthma and mortality increased in those with BMI ≤25; it was unclear if this association was statistically significant.(11)
Table 4. Data from primary studies on whether COVID-19 outcomes in PWA differ based on subgroup characteristics. Arrows indicate direction of association; double arrows indicate statistical significance[8]
| Study ID |
Age |
Medication |
Asthma severity/ type/ co-morbidities |
| Chhiba 2020(19) |
|
ICU admission
↑ ICS |
|
| Choi 2020(16) |
|
ICU admission
↑ ICS
↓ LABA
↓ SABA
↔LAMA
Mortality
↑ ICS
↔ LABA
↑ SABA
↓LAMA |
Mortality:
Asthma severity ↔ |
| Kim 2020(11) |
Mortality
Association between asthma and mortality ↑ with increasing age |
|
|
| Keswani 2020(14) |
|
|
ICU admission
↓ Allergic asthma (compared to non-allergic asthma) |
| Mahdavinia 2020(15) |
OR for association between asthma and hospitalisation ↑ with increasing age
OR for association between asthma and ICU admission less clear by age (association ↑ is those aged 50-64 compared to those aged 18-49 or 65+) |
|
|
| Schultze 2020(22) |
|
Mortality[9]
Compared to SABA:
↑ low/medium dose ICS
↑↑ high dose ICS |
|
| Wang 2020(21) |
Increasing age:
↑↑ Hospitalisation
↔ ICU admission
↑↑ Mortality |
Hospitalisation:
↓ ICS
↑ ICS-LABA
ICU admission:
↓ ICS
↓ ICS-LABA
Mortality:
↓ ICS
↓ ICS-LABA |
Hospitalisation:
↑↑ COPD
ICU admission:
↑ COPD
Mortality:
↑ COPD |
| Williamson 2020(18) |
|
Mortality
↑ OCS use |
|
| Yang 2020(12) |
|
|
↓↓ Allergic asthma (compared to non-allergic asthma)
Severe clinical outcomes (composite scores)
↓↓Allergic asthma (compared to non-allergic asthma) |
| Zhu 2020(13) |
|
|
↓ Allergic asthma (compared to non-allergic asthma)
↑ COPD |
Conclusion: It is unclear whether certain characteristics affect the association between asthma and COVID-19 outcomes. Systematic reviews have not investigated this. When evaluating relationships between asthma medications and increased risk, it is difficult to determine the extent to which any observed associations are driven by asthma severity.
Discussion
Whether PWA increases risk of infection or severe outcomes from COVID-19 remains unclear. There is no consensus from systematic reviews, and high quality primary studies report conflicting results in some areas. Within PWA with COVID-19, people with co-morbid COPD and people with non-allergic asthma appear more vulnerable to worse outcomes. Older age and non-white ethnicity also appear to confer greater risk within PWA, as would be expected from data from the general population. Data on asthma medication use is difficult to interpret due to inconsistent findings across primary studies and possible confounding/co-linearity between asthma severity and medication prescribed, though the largest study of its type found that ICS use was associated with higher mortality risk in PWA.(22) Further primary studies and comprehensive meta-analyses are needed.
As well as – and perhaps linked to- the conflicting and imprecise results noted above, there a number of other important limitations to evidence in this area. As described above, establishing risk of contracting COVID-19 remains extremely difficult without widespread community testing programmes which include asymptomatic individuals. Data on risk of contracting infection is therefore driven primarily by data from hospitals, where multiple biases are possible; e.g. studies which find higher rates of COVID-19 hospitalisation in PWA could be because PWA are more likely to contract COVID-19, or because if having contracted COVID-19 PWA are more likely to require hospitalisation or to be referred to hospital as a precautionary measure; studies which find lower rates of asthma in people hospitalised with COVID-19 could be because PWA have practiced increased protective measures, e.g. shielding, or because of incomplete recording of asthma status. Publication and reporting bias may be substantial issues; in primary studies which seek to evaluate risk factors for COVID-19, authors may evaluate long lists of possible predictors, but in their results only highlight those where statistically significant differences are found. The lack of clear data on whether there is an association between asthma and COVID-19 outcomes may also discourage research investigating whether specific characteristics within PWA (e.g. disease severity; medications) are associated with increased risk. Finally, none of the included studies evaluated the risk of persistence of COVID-19 symptoms (Long COVID) in PWA, meaning ‘severity’ measures only included hospitalisation and ICU.(23) In addition, none of the included studies looked at asthma control in the context of COVID-19 risk, with the exception of Williamson which found prescription of a recent dose of OCS was associated with increased risk in PWA compared to people without asthma.(18) Asthma control test scores have been found to be predictive of future asthma exacerbations, and future studies may want to consider these as potential explanatory variables for symptomatic COVID-19.(24, 25)
Some of the above limitations are relevant to all research into risks from COVID-19 in people with specific NCDs (e.g. establishing risk of contracting versus being hospitalised with COVID-19; imprecision due to this being an ever emerging research field). Of note, though, clear associations have emerged for other NCDs; for example, the link between diabetes and worse outcomes from COVID-19 is now broadly considered well-established.(26) Therefore, though the absence of evidence of a clear association between asthma and worse outcomes from COVID-19 should not be interpreted as evidence of absence, the data reviewed does give some indication that risks in PWA, as a whole, may be less than originally anticipated.
More research is clearly needed both on risks in PWA overall and in risks based on asthma phenotype, medication, and other characteristics. This data is needed to inform not only guidance on shielding and avoidance measures, but also is now acutely relevant to the prioritisation of different groups in regards to COVID-19 vaccination. Whilst awaiting further evidence, it is imperative that the evidence that is available now is transparently communicated to stakeholders to enable informed decision-making.
References
- Hartmann-Boyce J, Gunnell J, Drake J, Otunla A, Suklan J, Schofield E, et al. Asthma and COVID-19: review of evidence on risks and management considerations. BMJ Evid Based Med. 2020.
- PROTOCOL Rapid reviews of evidence for WHO scientific briefs on COVID-19 and selected Noncommunicable Diseases (NCDs) 2020 [Available from: https://www.cebm.net/covid-19/protocol-rapid-reviews-of-evidence-for-who-scientific-briefs-on-covid-19-and-selected-noncommunicable-diseases-ncds/.
- Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008.
- Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Oxford; 2000.
- Al-Shamrani A, Al-Harbi AS, Alhaider SA, Alharbi S, Al-Harbi NS, Alanazi A, et al. Approach to childhood asthma in the era of COVID-19: The official statement endorsed by the Saudi Pediatric Pulmonology Association (SPPA). Int J Pediatr Adolesc Med. 2020;7(3):103-6.
- Castro-Rodriguez JA, Forno E. Asthma and COVID-19 in children: A systematic review and call for data. Pediatr Pulmonol. 2020;55(9):2412-8.
- Wang Y, Chen J, Chen W, Liu L, Dong M, Ji J, et al. Does asthma increase the mortality of patients with COVID-19?: a systematic review and meta-analysis. Int Arch Allergy Immunol. 2020:1-7.
- Broadhurst R, Peterson R, Wisnivesky JP, Federman A, Zimmer SM, Sharma S, et al. Asthma in COVID-19 hospitalizations: an overestimated risk factor? Ann Am Thorac Soc. 2020;17(12):1645-8.
- Morais-Almeida M, Pité H, Aguiar R, Ansotegui I, Bousquet J. Asthma and the coronavirus disease 2019 Pandemic: a literature review. Int Arch Allergy Immunol. 2020;181(9):680-8.
- Atkins JL, Masoli JAH, Delgado J, Pilling LC, Kuo CL, Kuchel GA, et al. Preexisting Comorbidities Predicting COVID-19 and Mortality in the UK Biobank Community Cohort. J Gerontol A Biol Sci Med Sci. 2020;75(11):2224-30.
- Kim S, Jung CG, Lee JY, Kim G, Choi SW, Jin HJ, et al. Characterization of asthma and risk factors for delayed SARS-CoV-2 clearance in adult COVID-19 inpatients in Daegu. Allergy. 2020.
- Yang JM, Koh HY, Moon SY, Yoo IK, Ha EK, You S, et al. Allergic disorders and susceptibility to and severity of COVID-19: A nationwide cohort study. J Allergy Clin Immunol. 2020;146(4):790-8.
- Zhu Z, Hasegawa K, Ma B, Fujiogi M, Camargo CA, Jr., Liang L. Association of asthma and its genetic predisposition with the risk of severe COVID-19. J Allergy Clin Immunol. 2020;146(2):327-9.e4.
- Keswani A, Dhana K, Rosenthal JA, Moore D, Mahdavinia M. Atopy is predictive of a decreased need for hospitalization for coronavirus disease 2019. Ann Allergy Asthma Immunol. 2020;125(4):479-81.
- Mahdavinia M, Foster KJ, Jauregui E, Moore D, Adnan D, Andy-Nweye AB, et al. Asthma prolongs intubation in COVID-19. J Allergy Clin Immunol Pract. 2020;8(7):2388-91.
- Choi YJ, Park JY, Lee HS, Suh J, Song JY, Byun MK, et al. Effect of asthma and asthma medication on the prognosis of patients with COVID-19. Eur Respir J. 2020.
- Grandbastien M, Piotin A, Godet J, Abessolo-Amougou I, Ederlé C, Enache I, et al. SARS-CoV-2 pneumonia in hospitalized asthmatic patients did not induce severe exacerbation. J Allergy Clin Immunol Pract. 2020;8(8):2600-7.
- Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, et al. OpenSAFELY: factors associated with COVID-19 death in 17 million patients. Nature. 2020.
- Chhiba KD, Patel GB, Vu THT, Chen MM, Guo A, Kudlaty E, et al. Prevalence and characterization of asthma in hospitalized and nonhospitalized patients with COVID-19. J Allergy Clin Immunol. 2020;146(2):307-14.e4.
- Santos MM, Lucena EES, Lima KC, Brito AAC, Bay MB, Bonfada D. Survival and predictors of deaths of patients hospitalised due to COVID-19 from a retrospective and multicentre cohort study in Brazil. Epidemiol Infect. 2020;148:e198.
- Wang L, Foer D, Bates DW, Boyce JA, Zhou L. Risk factors for hospitalization, intensive care, and mortality among patients with asthma and COVID-19. J Allergy Clin Immunol. 2020;146(4):808-12.
- Schultze A, Walker AJ, MacKenna B, Morton CE, Bhaskaran K, Brown JP, et al. Risk of COVID-19-related death among patients with chronic obstructive pulmonary disease or asthma prescribed inhaled corticosteroids: an observational cohort study using the OpenSAFELY platform. Lancet Respir Med. 2020;8(11):1106-20.
- Yelin D, Wirtheim E, Vetter P, Kalil AC, Bruchfeld J, Runold M, et al. Long-term consequences of COVID-19: research needs. The Lancet Infectious Diseases. 2020;20(10):1115-7.
- Bateman ED, Reddel HK, Eriksson G, Peterson S, Ostlund O, Sears MR, et al. Overall asthma control: the relationship between current control and future risk. J Allergy Clin Immunol. 2010;125(3):600-8, 8.e1-8.e6.
- Przybyszowski M, Polczyk R, Sliwka A, Pilinski R, Wloch T, Nowobilski R, et al. Asthma Control Test (ACT) result as a predictor of asthma exacerbations. European Respiratory Journal. 2017;50(suppl 61):PA1124.
- Aggarwal G, Lippi G, Lavie CJ, Henry BM, Sanchis-Gomar F. Diabetes mellitus association with coronavirus disease 2019 (COVID-19) severity and mortality: A pooled analysis. J Diabetes. 2020;12(11):851-5.
Supplemental Tables
Supplemental Table 1. Key characteristics of included reviews[10]
Supplemental Table 2. AMSTAR-2 ratings for critical domains

Supplemental Table 3. Characteristics of cohort studies meeting threshold for contributing to outcomes estimates contributing to rapid review
APPENDIX 1 MEDLINE and EMBASE search terms
MEDLINE
| 1 |
exp Coronavirus/ |
| 2 |
exp Coronavirus Infections/ |
| 3 |
(coronavirus* or corona virus* or OC43 or NL63 or 229E or HKU1 or HCoV* or ncov* or covid* or sars-cov* or sarscov* or Sars-coronavirus* or Severe Acute Respiratory Syndrome Coronavirus*).mp. |
| 4 |
((pneumonia or covid* or coronavirus* or corona virus* or ncov* or 2019-ncov or sars*).mp. or exp pneumonia/) and Wuhan.mp. |
| 5 |
(2019-ncov or ncov19 or ncov-19 or 2019-novel CoV or sars-cov2 or sars-cov-2 or sarscov2 or sarscov-2 or Sars-coronavirus2 or Sars-coronavirus-2 or SARS-like coronavirus* or coronavirus-19 or covid19 or covid-19 or covid 2019 or ((novel or new or nouveau) adj2 (CoV on nCoV or covid or coronavirus* or corona virus or Pandemi*2)) or ((covid or covid19 or covid-19) and pandemic*2) or (coronavirus* and pneumonia)).mp. |
| 6 |
COVID-19.rx,px,ox. or severe acute respiratory syndrome coronavirus 2.os. |
| 7 |
1 or 2 or 3 or 4 or 5 or 6 |
| 8 |
exp Asthma/ |
| 9 |
asthma*.ti,ab,kw. |
| 10 |
8 or 9 |
| 11 |
exp Mortality/ |
| 12 |
exp Hospitalization/ |
| 13 |
Life Support Care/ |
| 14 |
exp Respiration, Artificial/ |
| 15 |
Critical Care/ |
| 16 |
intensive care units/ or respiratory care units/ |
| 17 |
incidence/ or prevalence/ or risk factors/ |
| 18 |
(mortality or death? or fatal* or survival or recovery).ti,ab,kw. |
| 19 |
((sever* or serious* or critical*) adj3 (infection* or complication* or ill*)).ti,ab,kw. |
| 20 |
(hospitali?ed or hospitali?ation*).ti,ab,kw. |
| 21 |
((hospital? or patient?) adj2 (admit* or admission* or readmit* or re-admit* or readmission* or re-admission* or discharg*)).ti,ab,kw. |
| 22 |
(life support or intubat* or ventilat*).ti,ab,kw. |
| 23 |
((artificial or assist*) adj2 (respiration or breathing)).ti,ab,kw. |
| 24 |
(critical care or intensive care or itu or icu or ccu).ti,ab,kw. |
| 25 |
(((prevalence or incidence) and (risk? or factor? or predict*)) or risk factor?).ti,ab,kw. |
| 26 |
((positive or negative or confirmed) adj2 case?).ti,ab,kw. |
| 27 |
((clinical or physical or patient?) adj2 (presentation or feature? or characteristic? or manifestation?)).ti,ab,kw. |
| 28 |
(presentation or feature? or characteristic? or manifestation?).ti. |
| 29 |
11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 |
| 30 |
7 and 10 and 29 |
| 31 |
limit 30 to yr=”2019 -Current” |
EMBASE
| 1 |
exp Coronavirus/ |
| 2 |
exp Coronavirus Infections/ |
| 3 |
(coronavirus* or corona virus* or OC43 or NL63 or 229E or HKU1 or HCoV* or ncov* or covid* or sars-cov* or sarscov* or Sars-coronavirus* or Severe Acute Respiratory Syndrome Coronavirus*).mp. |
| 4 |
((pneumonia or covid* or coronavirus* or corona virus* or ncov* or 2019-ncov or sars*).mp. or exp pneumonia/) and Wuhan.mp. |
| 5 |
(2019-ncov or ncov19 or ncov-19 or 2019-novel CoV or sars-cov2 or sars-cov-2 or sarscov2 or sarscov-2 or Sars-coronavirus2 or Sars-coronavirus-2 or SARS-like coronavirus* or coronavirus-19 or covid19 or covid-19 or covid 2019 or ((novel or new or nouveau) adj2 (CoV on nCoV or covid or coronavirus* or corona virus or Pandemi*2)) or ((covid or covid19 or covid-19) and pandemic*2) or (coronavirus* and pneumonia)).mp. |
| 6 |
1 or 2 or 3 or 4 or 5 |
| 7 |
exp Asthma/ |
| 8 |
asthma*.ti,ab,kw. |
| 9 |
7 or 8 |
| 10 |
exp Mortality/ or mortality risk/ |
| 11 |
survival/ or cause specific survival/ or long term survival/ or overall survival/ or survival factor/ or survival rate/ |
| 12 |
hospital admission/ or hospital discharge/ or hospital readmission/ or hospital utilization/ or hospitalization/ |
| 13 |
intensive care/ or exp artificial ventilation/ |
| 14 |
intensive care unit/ or medical intensive care unit/ |
| 15 |
incidence/ or prevalence/ or risk factor/ |
| 16 |
(mortality or death? or fatal* or survival or recovery).ti,ab,kw. |
| 17 |
((sever* or serious* or critical*) adj3 (infection* or complication* or ill*)).ti,ab,kw. |
| 18 |
(hospitali?ed or hospitali?ation*).ti,ab,kw. |
| 19 |
((hospital? or patient?) adj2 (admit* or admission* or readmit* or re-admit* or readmission* or re-admission* or discharg*)).ti,ab,kw. |
| 20 |
(life support or intubat* or ventilat*).ti,ab,kw. |
| 21 |
((artificial or assist*) adj2 (respiration or breathing)).ti,ab,kw. |
| 22 |
(critical care or intensive care or itu or icu or ccu).ti,ab,kw. |
| 23 |
(((prevalence or incidence) and (risk? or factor? or predict*)) or risk factor?).ti,ab,kw. |
| 24 |
((positive or negative or confirmed) adj2 case?).ti,ab,kw. |
| 25 |
((clinical or physical or patient?) adj2 (presentation or feature? or characteristic? or manifestation?)).ti,ab,kw. |
| 26 |
(presentation or feature? or characteristic? or manifestation?).ti. |
| 27 |
10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 |
| 28 |
6 and 9 and 27 |
| 29 |
limit 28 to yr=”2019 -Current” |
Figure 1. PRISMA diagram of study flow
APPENDIX 2. Primary studies identified which do not meet threshold for contributing to outcomes estimates
| Citation |
Study Type |
Study objective as
stated by authors |
Country |
Setting |
Study dates |
Participants |
Total number of
participants |
Outcomes reported |
| Abrams MP, Wan EY, Waase MP, et al. Clinical and cardiac characteristics of COVID‐19 mortalities in a diverse New York City Cohort. J Cardiovasc Electrophysiol. 2020; 1–11. DOI: 10.1111/jce.14772 |
Retrospective cohort study |
Pertain to arrhythmic vs non-arrhythmic deaths not relevant for this review. |
USA |
Hospital |
Between March 1 and April 3, 2020 |
Adults |
Total: 6310
Asthma: 577 |
Mortality |
| Adrish M, Chilimuri S, Sun H, et al. (September 03, 2020) The Association of Renin-Angiotensin-Aldosterone System Inhibitors With Outcomes Among a Predominantly Ethnic Minority Patient PopulationHospitalized With COVID-19: The Bronx Experience. Cureus 12(9): e10217. DOI 10.7759/cureus.10217 |
Retrospective cohort study |
In this study, we aimed to examine the characteristics of the COVID-19-positive patients who were hospitalised during the peak of the pandemic and whether the use of ACE/ARB affected their treatment outcomes. |
USA |
Hospital |
March 1, 2020,to March 31, 2020 |
Adults |
Asthma population: 212
Asthma plus probable COVID-19: 29
Asthma no COVID-19: 183 |
Prevalence |
| Barroso B, Valverde-Monge M, Canas JA, Rodrigo-Munoz JM, et al. resenting prevalence, characteristics and outcome of asthmatic patients with T2 diseases in hospitalized subjects with COVID-19 in Madrid, Spain. Journal of Investigational Allergology & Clinical Immunology 2020;30(5). doi: 10.18176/jiaci.0627 |
Retrospective cohort study |
We aim to report the prevalence of asthma and T2 diseases on a sample of hospitalized patients with COVID-19. |
Spain |
Hospital |
between March 1st and March 21st, 2020. |
Adult |
445 |
Prevalence, ICU admission, deaths |
| Beurnier A, Jutant E-M, Jevnikar M, et al. Characteristics and outcomes of asthmatic patients with COVID-19 pneumonia who require hospitalisation. Eur Respir J 2020; in press (https://doi.org/10.1183/13993003.01875-2020). |
Prospective cohort |
The objective of this study was to investigate the characteristics and outcomes of asthmatic patients with COVID-19 pneumonia who required hospitalization during the spring 2020 outbreak in Paris, France. |
France |
Hospital |
March 15, 2020 to April 15, 2020 |
Adult |
Whole cohort: 11405
Self reported asthma: 618 |
Prevalence |
| Bozek A, Winterstein J. Montelukast’s ability to fight COVID-19 infection, Journal of Asthma, 2020. DOI: 10.1080/02770903.2020.1786112 |
Retrospective cohort study |
To determine whether Montelukast can be effective in the treatment of SARS-CoV-2 infection. |
Poland and Germany |
Two outpatient clinics |
March to April 2020 |
Adults (elderly >60 years) |
COVID-19 mortality: 133 |
Prevalence and hospitalisations by medication group |
| Broadhurst R, Peterson R, Wisnivesky JP, Federman A, et al. Asthma in COVID-19 Hospitalizations: An Overestimated Risk Factor? Annals of the American Thoracic Society 2020;31(ANNALSATS Articles in Press. Published August 31, 2020 as 10.1513/AnnalsATS.202006-613RL) |
cross-sectional |
Using a cross sectional analysis of 436 COVID-19 patients admitted to the University of Colorado Hospital, we evaluated the likelihood of intubation in asthmatics compared to non-asthmatics. |
USA |
Hospital |
Not stated |
Not stated |
Total COVID-19 positive: 469
ACE/ARB group: 91
Non-ACE/ARB group: 378 |
ICU admission (univariate), Intubation (multivariate) |
| Garcia-Pachon, E.; Zamora-Molina, L.; Soler-Sempere, M. J.; et al. Asthma prevalence in patients with SARS-CoV-2 infection detected by RT-PCR not requiring hospitalization. Respiratory Medicine 2020;171():106084. https://doi.org/10.1016/j.rmed.2020.106084 |
Retrospective cohort study |
The objective of this study was to analyze the presence of asthma in a consecutive series of patients who tested positive in the RT-PCR assay for SARS-CoV-2 and did not require hospital admission. |
Spain |
Community and hospitalised patients. |
from March 3 to April 12, 2020. |
adult (although included from aged 14) |
Asthma group: 11
Non-asthma group: 178 |
Prevalence, hospitalisation |
| Hashim, M. J.; Alsuwaidi, A. R.; Khan, G. Population Risk Factors for COVID-19 Mortality in 93 Countries. Journal of Epidemiology and Global Health 2020;10(3):204-208. https://doi.org/10.2991/jegh.k.200721.001 |
Cross-sectional analysis |
In this study, we aimed to examine Case Mortality Rates (CMR) for 93 countries against eight diseases and six sociodemographic factors. |
Global – 93 countries |
CMR – database analysis |
Not stated but article accepted in July 2020 |
Not stated, vast majority likely to be adult |
Total hospitalised: 768
Asthma group: 37 |
Mortality |
Ko, J. Y.; Danielson, M. L.; Town, M.; et al.; Covid-Net Surveillance Team
Risk Factors for COVID-19-associated hospitalization: COVID-19-Associated Hospitalization Surveillance Network and Behavioral Risk Factor Surveillance System. Clinical Infectious Diseases 2020;18. doi/10.1093/cid/ciaa1419/5908300 |
Cross-sectional analysis |
We sought to identify factors independently associated with COVID-19-associated hospitalizations. |
USA |
Hospital, data from BPFSS community based in same catchment areas used for weighting |
March 1–June 23, 2020 |
Adult |
436 hospitalised COVID-19 patients
asthma group: 53
no asthma group: 383 |
Hospitalisation |
| Lemus Calderon JA, Martin PB, Rodriguez RG, et al. Differentiating characteristics of patients with asthma in thesevere acute respiratory syndrome coronavirus 2 infection. American College of Allergy, Asthma & Immunology. 2020. https://doi.org/10.1016/j.anai.2020.09.0041081-1206 |
Retrospective cohort study |
The main objective of our study was to analyze how the SARS-CoV-2 infection has affected patients with asthma in terms of prevalence, morbidity, hospitalisation, and mortality. |
Spain |
Hospital and community |
Data up to July 2020 |
Not stated |
Total COVID-19 positive: 376 |
Prevalence, hospitalisations, mortality. |
| Lieberman-Cribbin W, Rapp J, Alpert N, et al. The Impact of Asthma on Mortality in Patients With COVID-19. Chest 2020. DOI:https://doi.org/10.1016/j.chest.2020.05.575 |
Retrospective cohort study |
We describe results from the Mount Sinai Health System (MSHS) COVID-19 registry, with the objective to determine the prevalence of asthma in the MSHS COVID-19 registry and the association between a history of asthma and mortality. |
USA |
Hospital – inpatients and admissions to the ED |
February 29, 2020-April 24, 2020 |
Adults |
Not reported |
Prevalence and mortality, subgrouping by steroid use |
| Lombardi, C.; Roca, E.; Bigni, B.; et al. Clinical course and outcomes of patients with asthma hospitalized for severe acute respiratory syndrome coronavirus 2 pneumonia: A single-center, retrospective study. Annals of Allergy, Asthma, & Immunology 2020. https://doi.org/10.1016/j.anai.2020.07.029 |
Retrospective cohort study |
In this single-center, observational study, we investigated patients with asthma with confirmed SARS-CoV-2 pneumonia who were admitted to our hospital. |
Italy |
Hospital |
February 20, 2020 to April 20, 2020 |
Adult (for those with asthma) |
Total hospitalised: 5416
Number hospitalised with asthma: 702 |
prevalence, ICU admissions, deaths |
| Lovinsky-Desir, S.; Deshpande, D. R.; De, A.; Murray, Let al. Asthma among hospitalized patients with COVID-19 and related outcomes. Journal of Allergy & Clinical Immunology 2020. https://doi.org/10.1016/j.jaci.2020.07.026 |
Retrospective cohort study |
Given the high prevalence of asthma in the New York City area, our objective was to determine whether underlying asthma was associated with poor outcomes among hospitalized patients with severe COVID-19 compared with patients without asthma. |
USA |
Hospital |
between February 11, 2020, and May 7, 2020. |
Mixed (some subgrouping by age) |
Total: 1043
With asthma: 20 |
prevalence, ICU admissions, deaths |
| Matucci, A.; Caminati, M.; Vivarelli, V.; et al. COVID-19 in severe asthmatic patients during ongoing treatment with biologicals targeting type 2 inflammation: results from a multicenter Italian survey. Allergy 2020. DOI: 10.1111/all.14516 |
cross-sectional survey |
Data about the prevalence and severity of COVID-19 in asthma patients are very scarce, and no conclusive evidence is available. Additional concerns about the effects of asthma medications on SARS-CoV-2 infection may arise, and data about severe asthma during ongoing biological treatment in COVID-19 pandemic are lacking. |
Italy |
Telephone survey of asthma patients recruited from asthma centres across Italy |
April 1st, 2020 and April 20th, 2020. |
Recruited from asthma centres across Italy |
Total: 1298
No asthma: 1135
With asthma: 163 |
Prevalence, hospital and ICU admission |
| Niquini, R. P.; Lana, R. M.; Pacheco, A. G.; et al. Description and comparison of demographic characteristics and comorbidities in SARI from COVID-19, SARI from influenza, and the Brazilian general population. Cadernos de Saude Publica 2020;36(7):e00149420 |
cross-sectional analysis |
The current study aims to describe patients hospitalized for severe acute respiratory illness (SARI) due to COVID-19 (SARI-COVID) in Brazil, according to their demographic characteristics and comorbidities up to the 21st Epidemiological Week (EW) of 2020. The study also aims to compare these characteristics to those of patients hospitalized for SARI from influenza in 2019/2020 (SARI-FLU). |
Brazil |
Hospital (comparator general population) |
up to the 21st Epidemiological Week of 2020, ending on May 23, 2020 (first case confirmed in Brazil on February 26, 2020) |
Both paediatric and adult for whole hospitalised sample, all those with asthma were adults. |
473 with asthma and on biological therapy
4 with confirmed COVID-19 |
Prevalence |
| Nystad, Wenche; Hjellvik, Vidar; Larsen, Inger Kristin; et al. Underlying conditions in adults with COVID-19. Tidsskr Nor Laegeforen 2020. DOI: 10.4045/tidsskr.20.0512 |
cross-sectional analysis |
The purpose of this study is to describe how selected disease states are distributed among adults with proven covid-19 (covid-19-test-positive) and among inpatients (covid-19-inpatients) compared with the population. |
Norway |
Community and hospital (reported separately) |
1.3.2020–13.5.2020. |
Adult (20 and older) |
31962 patients hospitalised with COVID-19 |
Prevalence, hospitalisation |
| Papadopoulos, N. G.; Custovic, A.; Deschildre, A.; et al.; Pediatric Asthma in Real Life, Collaborators. Impact of COVID-19 on Pediatric Asthma: Practice Adjustments and Disease Burden. The Journal of Allergy & Clinical Immunology in Practice 2020;8(8):2592-2599.e3 |
cross-sectional analysis |
To describe the impact of the COVID-19 pandemic on pediatric asthma services and on disease burden in their patients. |
Global |
Online survey to members of the Pediatric Asthma in Real Life think tank and the World Allergy Organization Pediatric Asthma Committee. |
Invited to complete the survey on April 9, 2020 with up to 10 days to complete. |
Paediatric |
7632 COVID-19 positive
1025 COVID-19 positive inpatients |
Hospitalisation, ICU admission, deaths (all made a clinical recovery) |
| Ruano FJ, Somoza Álvarez ML, Haroun-Díaz E, et al. Impact of the COVID-19 pandemic in children with allergic asthma. J Allergy Clin Immunol Pract 2020;8(9):3172-4 |
Cross-sectional (timelines unclear) |
This study aims to determine the impact of SARS-CoV-2 infection among children with asthma in our allergy department during the pandemic. |
Spain |
Attendees of allergy department in Madrid |
February-April 2020 |
Paediatric |
Ninety-one experts, 15 patients |
Prevalence (probable COVID cases in asthma population) and subgrouping by asthma medications. |
| Song, J.; Zeng, M.; Wang, H.; et al. Distinct effects of asthma and COPD comorbidity on disease expression and outcome in patients with COVID-19. Allergy 2020. DOI: 10.1111/all.14517 |
Retrospective cohort study |
In this study, we studied the prevalence of asthma and COPD comorbidities, and their impact on the disease expression, immune and inflammatory reaction and treatment outcome in hospitalized COVID-19 patients in Wuhan, China. |
China |
Hospital |
February 1, 2020, to March 6, 2020 |
Adult |
Total: 961
Asthma: 22 |
Prevalence, mortality |
| Toussie, D.; Voutsinas, N.; Finkelstein, M.; et al. Clinical and Chest Radiography Features Determine Patient Outcomes in Young and Middle-aged Adults with COVID-19. Radiology 2020;297(1):E197-E206 |
Retrospective cohort study |
To analyze the prognostic value of a chest radiograph severity scoring system for younger (nonelderly) patients with COVID-19 at initial presentation to the emergency department (ED); outcomes of interest included hospitalization, intubation, prolonged stay, sepsis, and death. |
USA |
Hospital |
March 10th-26th, 2020 |
Adult |
338 |
Prevalence, radiograph score and outcomes reported for asthma patients |
[1] Note potential overlap of data in Atkins and Zhu, both include data from UK Biobank
[2] Propensity scores generated by multiple logistic regression using known risk factors for COVID-19 (age, sex, hypertension, diabetes, body mass index >30kg/m2, and heart failure) as independent variables
[3] Model 1 was adjusted for age and sex; Model 2 was adjusted for age, sex, body mass index, smoking history, underlying comorbidity (chronic obstructive pulmonary disease, diabetes, hypertension, heart failure, other heart disease, chronic kidney disease, chronic liver disease, cancer, autoimmune disease, dementia, and other psychological disorder), and medication (antiretroviral, hydroxychloroquine, systemic steroid, and azithromycin).
[4] adjusted for age group, sex, ethnicity, education, and baseline assessment centre
[5] adjusted for age group, sex, ethnicity, education, baseline assessment center, and all comorbidities
[6] Model 1 was adjusted for age and sex; Model 2 was adjusted for age, sex, body mass index, smoking history, underlying comorbidity (chronic obstructive pulmonary disease, diabetes, hypertension, heart failure, other heart disease, chronic kidney disease, chronic liver disease, cancer, autoimmune disease, dementia, and other psychological disorder), and medication (antiretroviral, hydroxychloroquine, systemic steroid, and azithromycin).
[7] adjusted for significant variables in the modelling (both statistically and theoretically significant, no further details)
[8] Associations are from fully-adjusted models, where multiple models reported
[9] Authors state: “Sensitivity analyses showed that the apparent harmful association we observed could be explained by relatively small health differences between people prescribed ICS and those not prescribed ICS that were not recorded in the database (e value lower 95% CI 1·43)”
[10] NS: not specified
[11] As stated by authors
[12] Note potential overlap of data in Atkins and Zhu, both include data from UK Biobank