The Declining Case Fatality Ratio in England
August 19, 2020
The CFR has fallen substantially from its peak in April. We now present data suggesting that the CFR as of the 4th of August stood at around 1.5%, having fallen from over 6% six weeks earlier.
Daniel Howdon, Carl Heneghan
The recent publication of statistics based on deaths following a COVID-19 positive test in the last 28 days allows the calculation of a daily-updated case fatality ratio (CFR) that better reflects the current state of the epidemic.
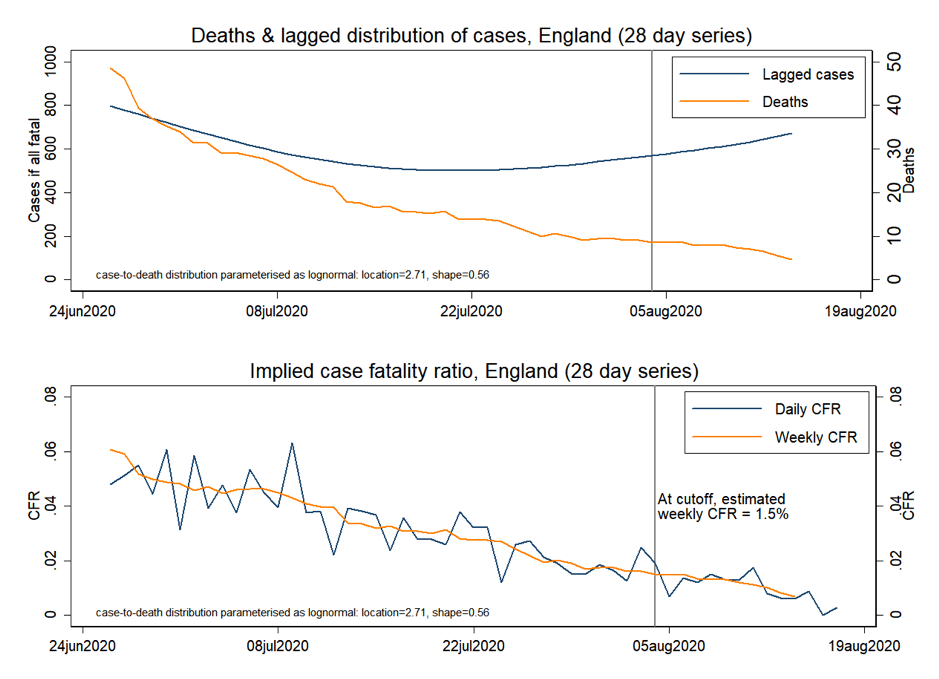
Using data published up to 18th of August, we derive the profile for the last eight weeks of deaths within 28 days of a positive test, cases (from the previous 28 days) lagged according to this distribution to provide an expected date of death were the case to prove fatal and the implied CFR.
The distribution of lagged cases stops falling and begins to rise around the 22nd of July, indicating when we would expect the deaths series to rise if cases were as fatal as previously.
The trend in deaths, however, continues downwards, indicating that the recent increase in cases is not leading to increased mortality. Figure 1 shows our estimate of the CFR as of the 4th of August as 1.5% – and seemingly still falling.
Figure 1
Methodological issues
Calculation of case fatality ratio requires both a count of relevant deaths and a count of relevant cases. While the count of each is unambiguous – the numbers published by the date of death (for deaths) and by date of the specimen (for cases) – further assumptions regarding the appropriate time lag between cases and deaths are required. The recent review by Public Health England reported that around 88% of deaths from COVID-19 occurred within 28 days of a positive test. We use this figure, along with an estimated distribution for the period from onset of symptoms to death derived from data held in the COVID-19 Hospitalisation in England Surveillance System (CHESS) and published in (Wood, 2020). We briefly consider the sensitivity of our estimates to other assumed distributions.
Wood (2020) reports that the distribution of onset of symptoms to death can be modelled by a log-normal distribution with a mean of 21 days and a standard deviation of 12.7 days. Compared with PHE’s estimates of 88% of deaths within 28 days, the use of such a distribution would correspond to around 78% of expected deaths within 28 days. As such, we use this distribution as a base and scale down the mean and standard deviation by a common factor to fit the proportion of deaths within 28 days to 88%. This implies the use of a lognormal distribution with mean 17.5 and standard deviation 10.6 (location parameter 2.71, shape 0.56), which forms our base case distribution.
While reporting lags based on the 28-day measure of COVID-19 deaths not yet apparent, we can infer, except in rare cases, that previous Public Health England numbers formed a near-complete record after 14 days – indeed in most cases, this lag was much shorter. We can, therefore, treat a 14 day-lagged measure of deaths as the point at which trends can be established with high confidence.
Explanations of the fall in the CFR
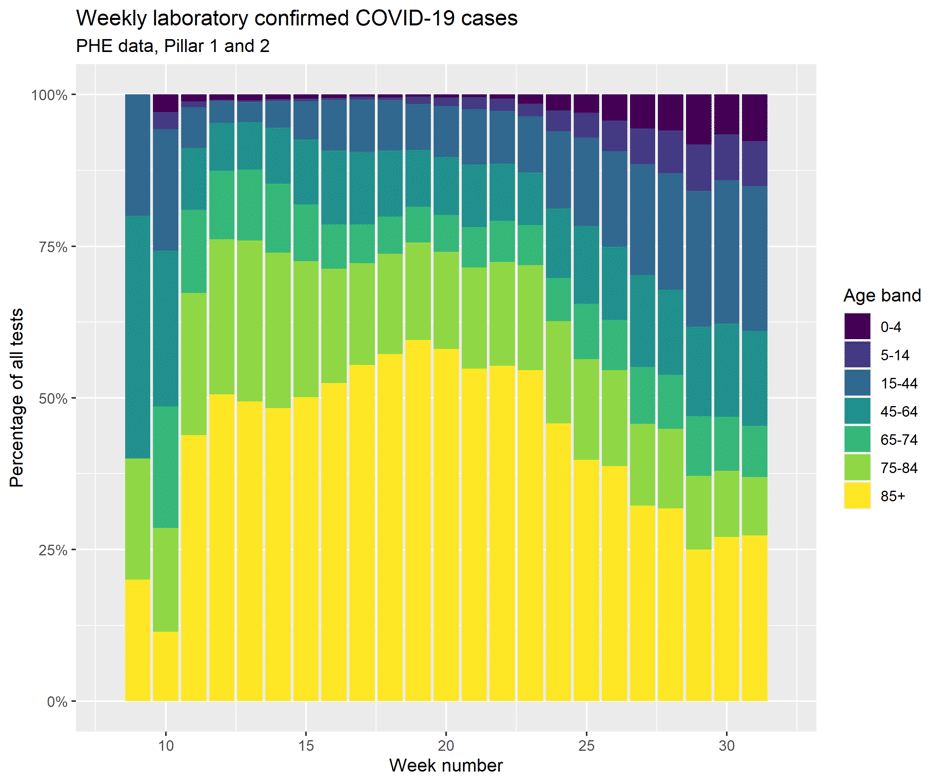
Explanations of this effect include the greater ascertainment of cases that were previously not being detected, and/or cases of equal severity now proving less fatal, due to perhaps improved treatment. The former is likely, given the ramping up of community testing and the recent trends in the age profile of detected cases being younger (See Figure 2)
Figure 2
While our CFR value is partly driven by the choice of distribution, results appear relatively robust. Assuming Wood (2020)’s symptoms-to-death distribution (implying only 78% of deaths within 28 days) yields an estimate of 1.69%, again falling. An alternative symptoms-to-death distribution parameterised on data from Stockholm yields an estimate of 1.4%, which is also falling.
We will update this series in coming weeks as this estimate of the CFR changes. In our next post, we will use similar methods to consider different estimates of the infection fatality ratio.
Reference
Wood, S. N. (2020). Did COVID-19 infections decline before UK lockdown? ArXiv:2005.02090 [q-Bio, Stat]. http://arxiv.org/abs/2005.02090
Daniel Howdon is a Researcher, Health Economics, LIHS UCU Department Representative, Academic Unit of Health Economics, University of Leeds. Bio here
Carl Heneghan is Professor of Evidence-Based Medicine, Director of the Centre for Evidence-Based Medicine and Director of Studies for the Evidence-Based Health Care Programme. (Full bio and disclosure statement here)
Disclaimer: the article has not been peer-reviewed; it should not replace individual clinical judgement, and the sources cited should be checked. The views expressed in this commentary represent the views of the authors and not necessarily those of the host institution, the NHS, the NIHR, or the Department of Health and Social Care. The views are not a substitute for professional medical advice.