Tracking mortality over time – ONS Update 5th May
May 5, 2020
Jason Oke, Nick DeVito, Carl Heneghan.
We are tracking the ONS data on deaths, which updates every Tuesday.
How can we tell if COVID-19 is the principal cause of these deaths? Or if they would have occurred in the absence of COVID-19, particularly in the elderly and people with chronic health problems? (see David Spiegelhalter’s article for an explanation).
One way is to examine the death rates and determine if more people are dying than we would expect. What we want to know is whether the reported COVID deaths represent an “excess” over the norm.
The weekly number of registered deaths for all ages.
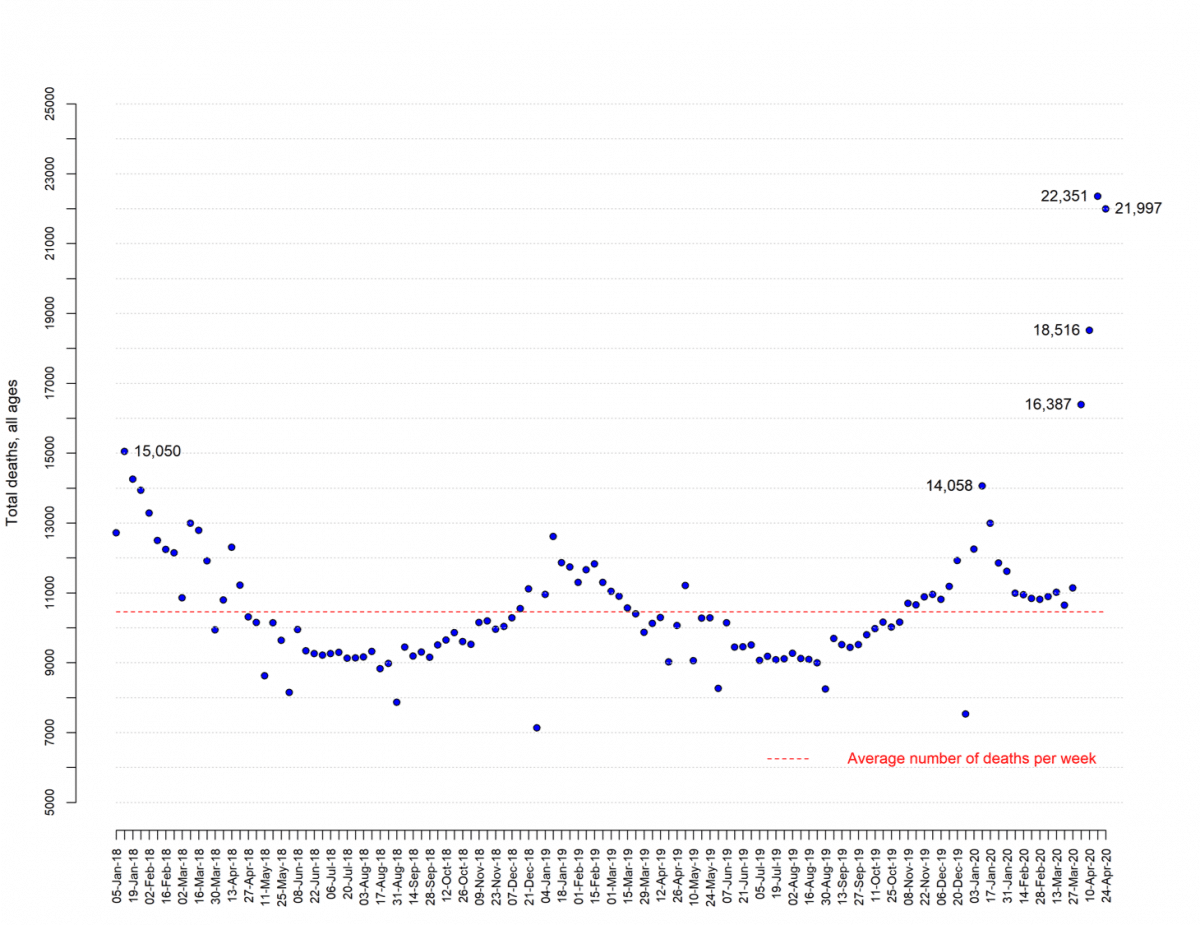
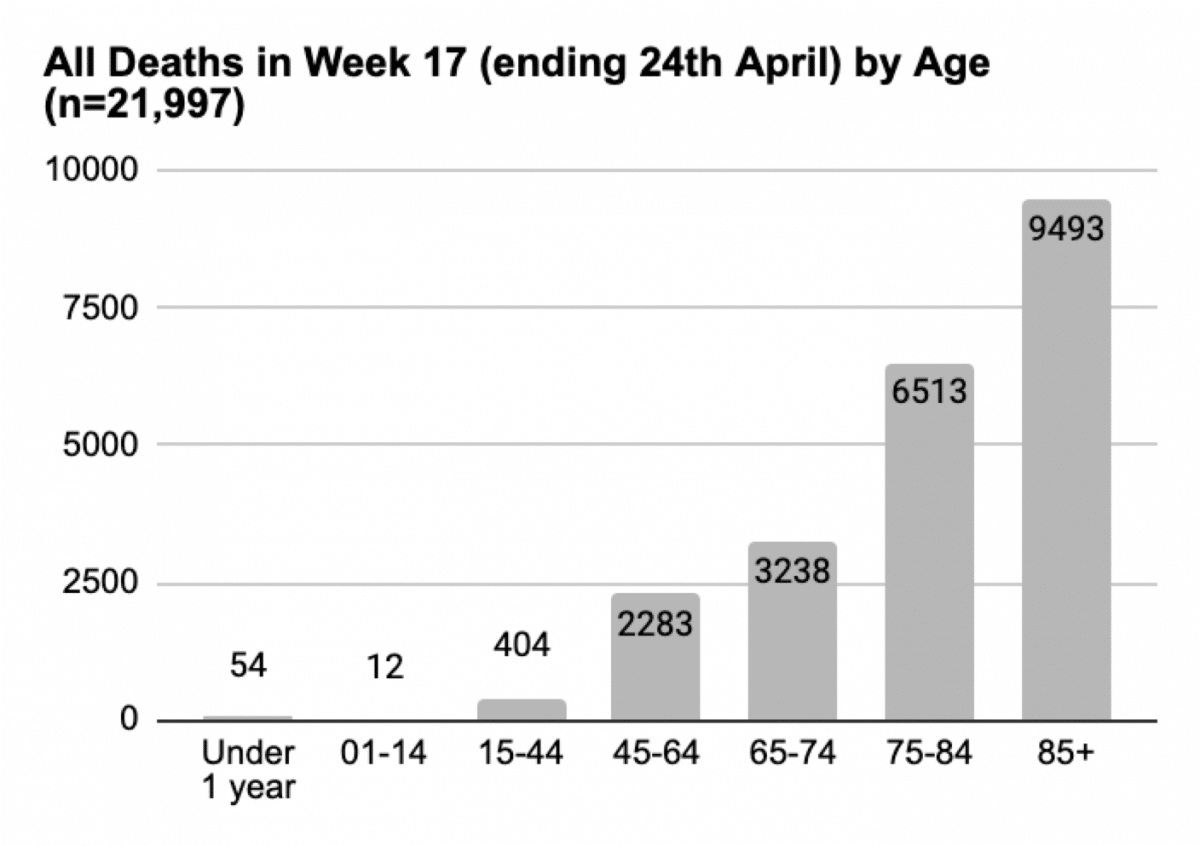
Update April 28th: today’s data release refers to the week ending the 24th of April (week 17)
- Total deaths all ages 21,997 deaths.
- This is an excess of 11,539 deaths over the average expected for this times of the year: more than double what is expected at this time of year, RR 2.10 (95% CI 2.05 to 2.15; p<0.0001).
- Since week 13 there has been an excess of 38,482.
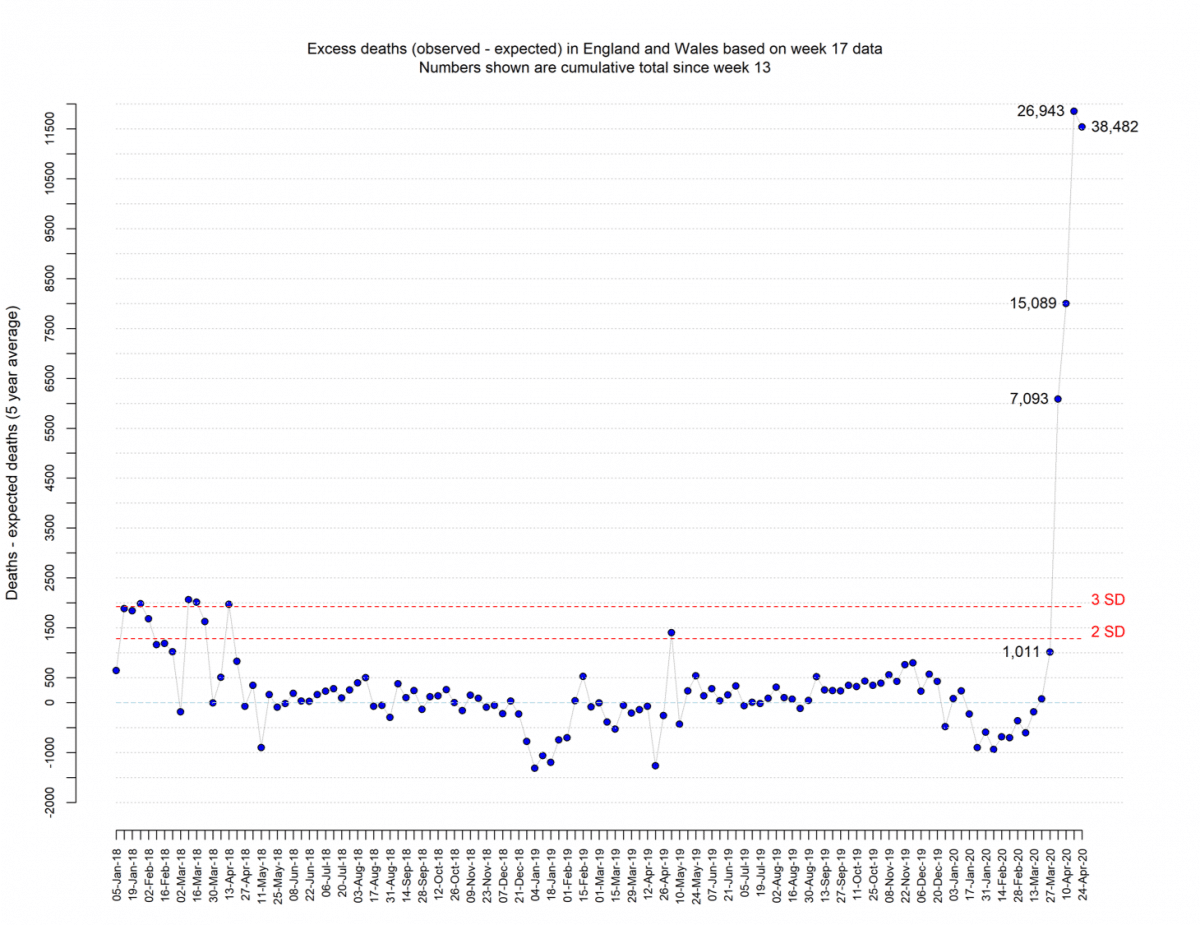
The number of deaths has exceeded 3 SDs on 5 separate occasions in the past three years. In the 2017 to 2018 winter period, there were 50,100 excess winter deaths in England and Wales. The highest previous recorded deaths (we are aware of) per week occurred in week 52 of 1999 when 18,500 deaths were registered in that week.
Were excess deaths due to COVID?
- In week 17, of the 11,539 excess deaths, 8,273 (72%) mentioned COVID on the death certificate, (28%) did not.
There are two possible explanations for why COVID is not mentioned on the death certificate:
- Underreporting of COVID on death certificates
- Deaths from other causes are going up
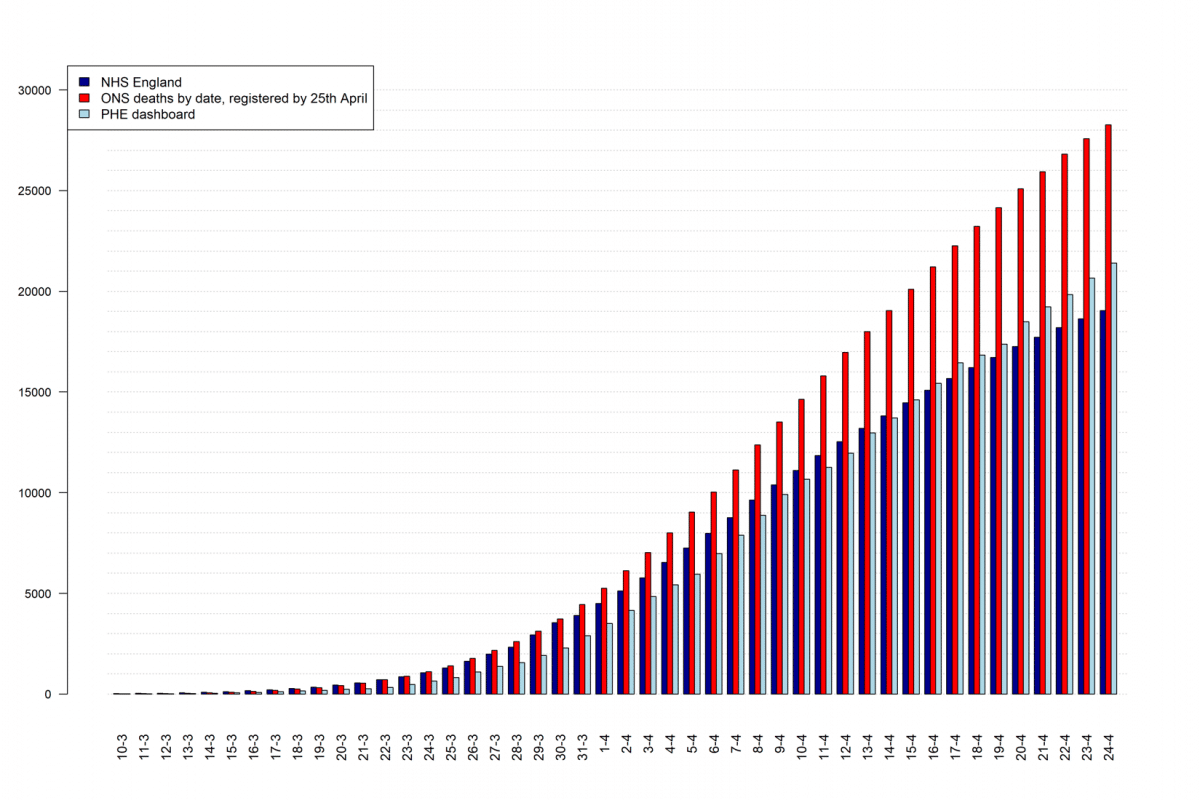
The peak of deaths is consistent with NHS England’s peak of deaths – the 8th of April.
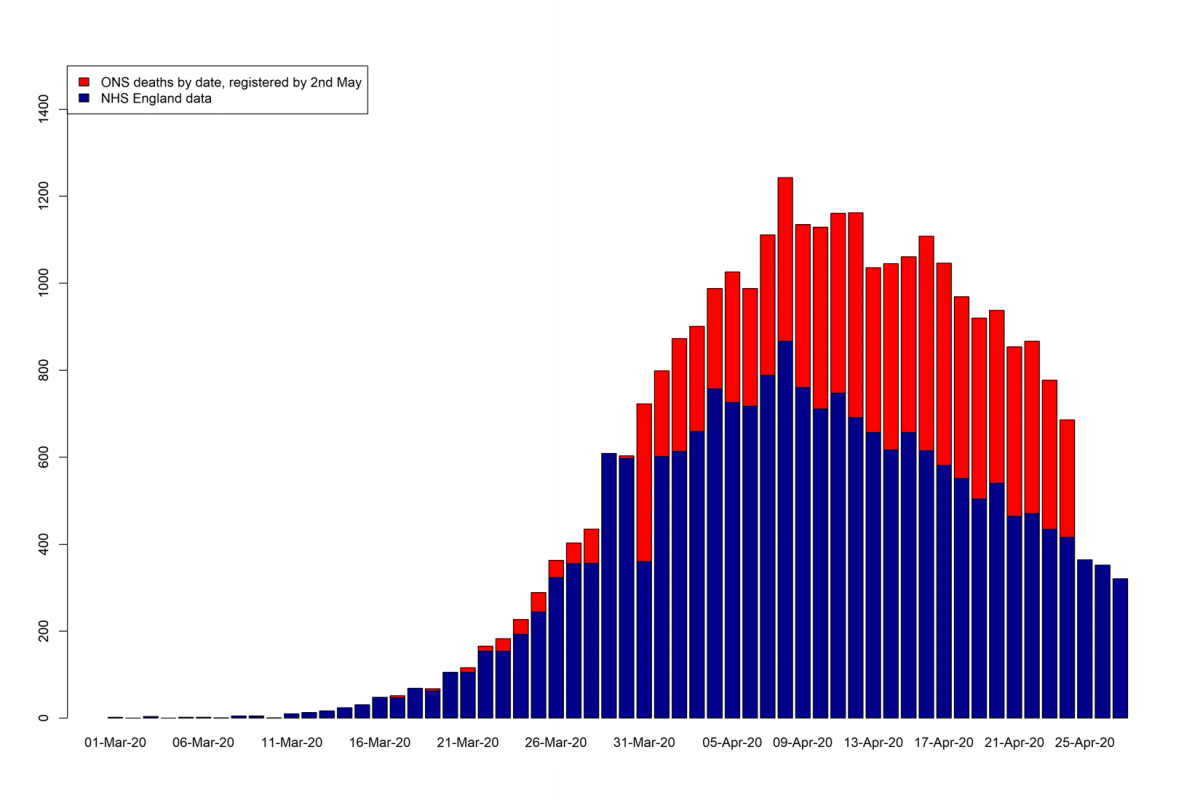
Cumulative numbers of deaths by different Data Source
Age of deaths
- 72.8% of all the deaths occurred in > 75-year olds
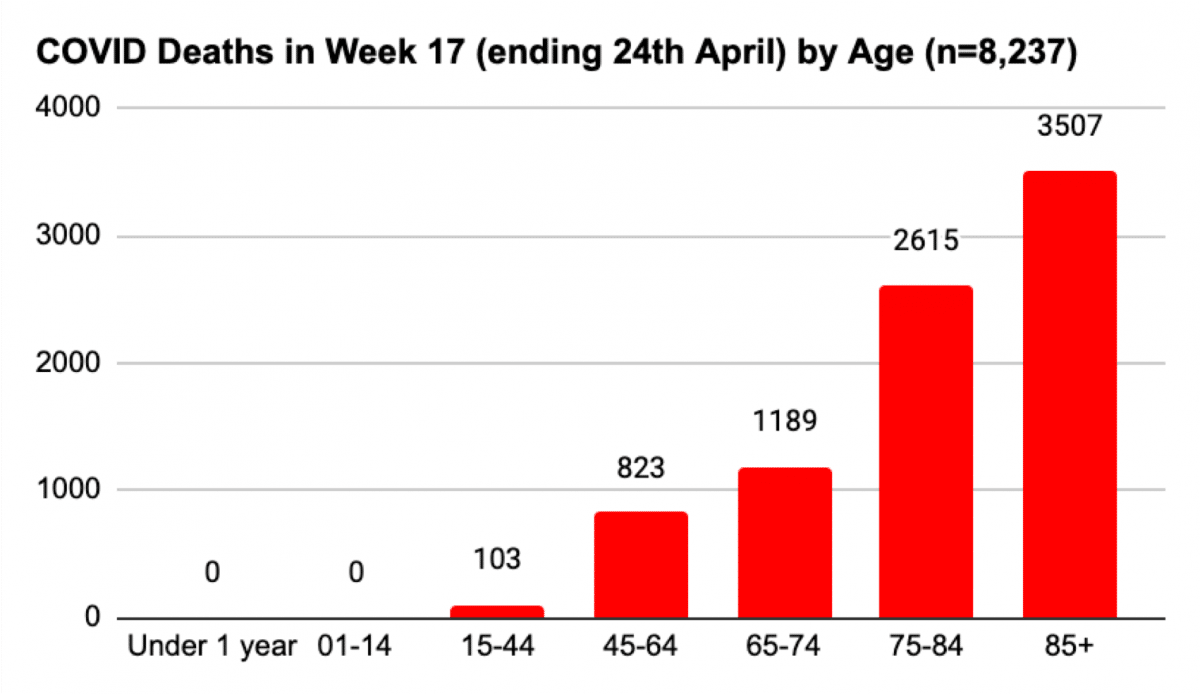
- 74.3% of COVID deaths occurred in > 75-year-olds (compared with 71.4% in week 16).
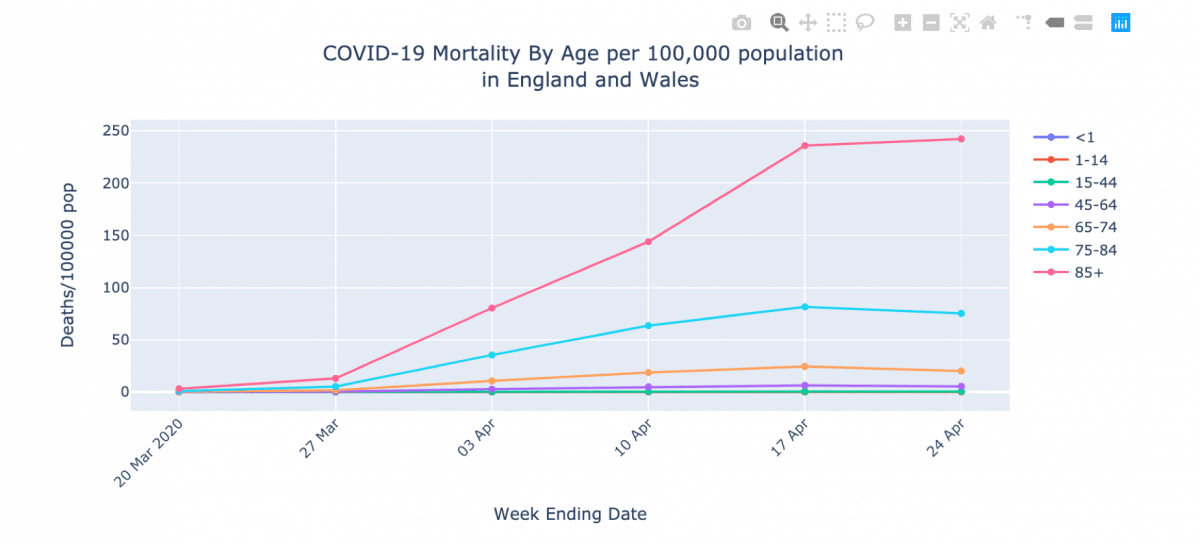
Interactive graphs for mortality by age per 100,000 population
it is important to look at the rates of death by age of the population at risk (there are fewer 85-year-olds than those in the 45 to 64 age group. What this does is show the much higher risk in the elderly compared to younger age groups
Mortality by Age per 100,000 population
- >85s: 242/100,000
- 75-84: 75 per 100,000
- 65-74: 20 per 100,000
- 45-64: 5.4 per 100,000
- 15-44: 0.46 per 100,000
The ONS reporting doesn’t tell us if COVID was mentioned as the disease or condition that led directly to the death.
- The immediate cause of death – (first line of the death certificate in Part I)
- The underlying causes of death – considers the chain of events leading ultimately to death (lowermost lines in Part I)
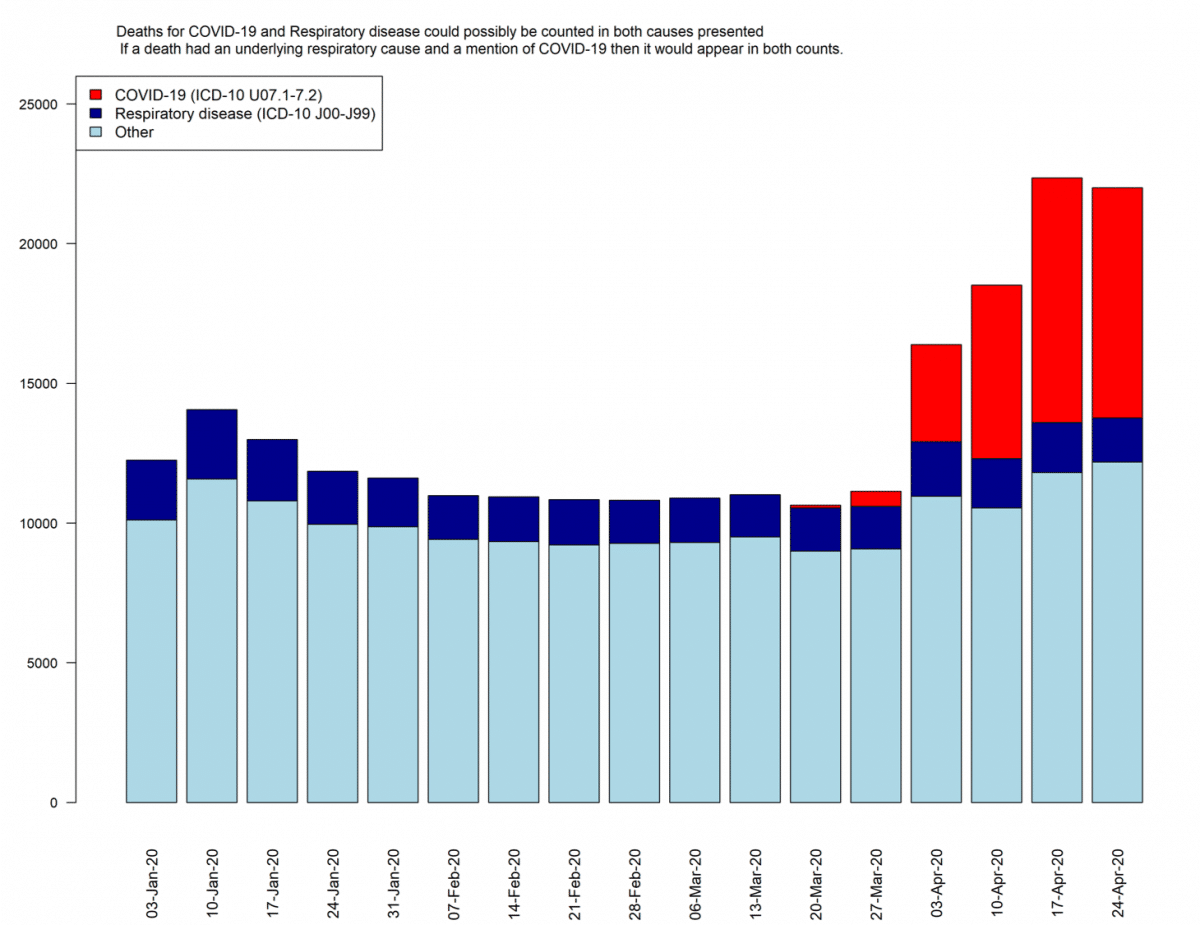
All respiratory diseases deaths (ICD-10 J00-J99)
This includes deaths from Viral pneumonia (coded as J12).
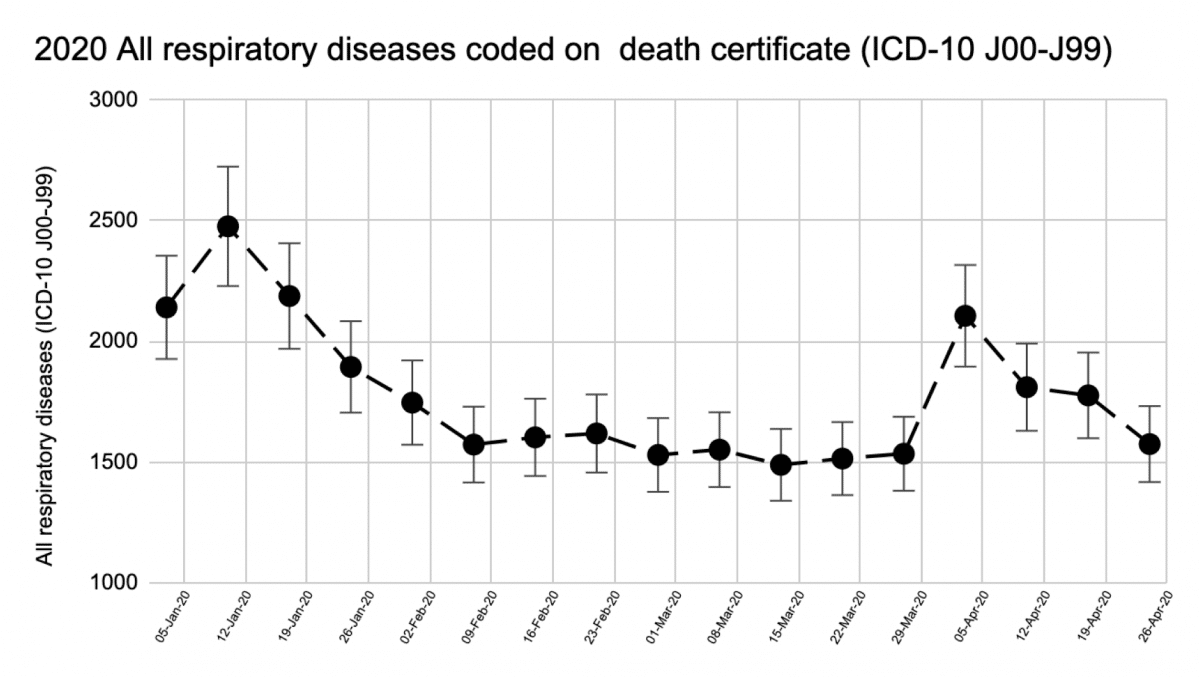
You would expect pneumonia to be on the rise if SARs-CoV-2 predominately caused viral pneumonia. A death certificate would contain both COVID and viral pneumonia if this was the case. The predominant cause of COVID deaths is not respiratory. Further in-depth analysis of ONS data can reveal the other causes.
Interactive graphs available here
Place of death
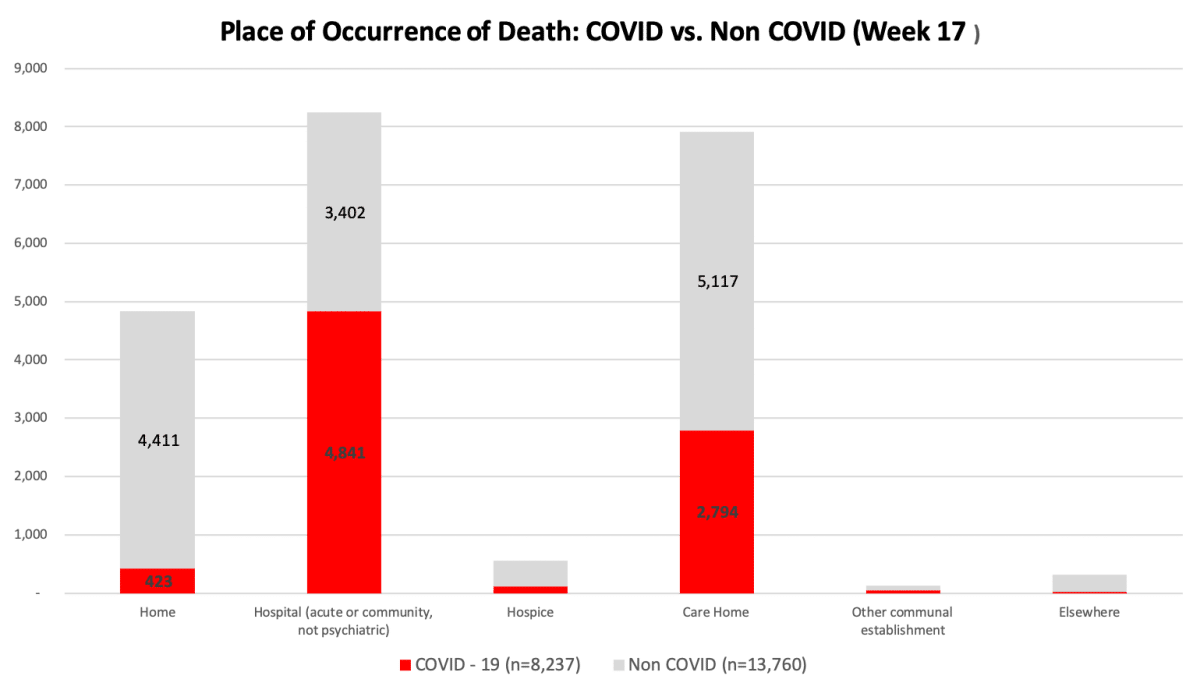
Deaths in care homes (n=7,911) and at home (n=4,834) added together were greater than the number of deaths in hospital (8,243).
There was a greater proportion of non-COVID deaths at home (91%) and care homes setting (65%) than COVID deaths.
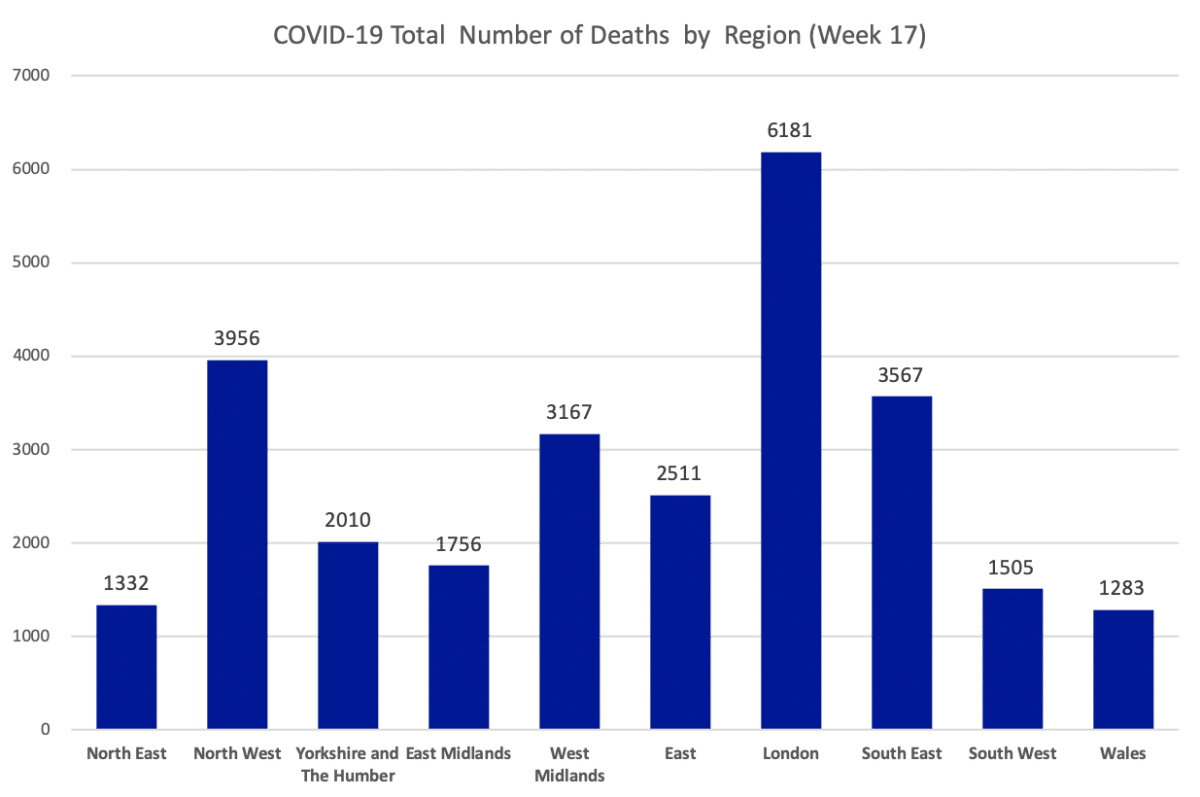
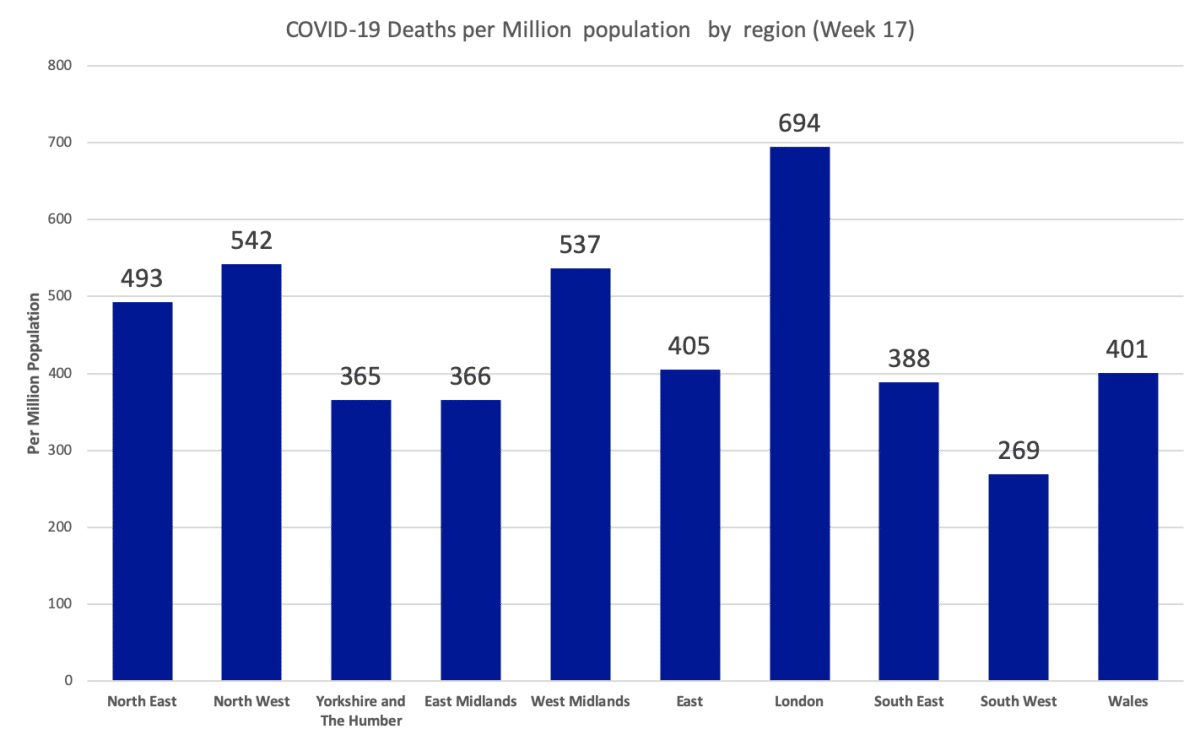
Deaths by Region
See also
AUTHORS
Jason Oke is a Senior Statistician at the Nuffield Department of Primary Care Health Sciences and Module Coordinator for Statistical Computing with R and Stata (EBHC Med Stats), and Introduction to Statistics for Health Care Research (EBHC), as part of the Evidence-Based Health Care Programme.
Nick DeVito is a Doctoral Researcher at the EBM DataLab.
Carl Heneghan is Professor of Evidence-Based Medicine, Director of the Centre for Evidence-Based Medicine and Director of Studies for the Evidence-Based Health Care Programme. (Full bio and disclosure statement here)
Disclaimer: the article has not been peer-reviewed; it should not replace individual clinical judgement, and the sources cited should be checked. The views expressed in this commentary represent the views of the authors and not necessarily those of the host institution, the NHS, the NIHR, or the Department of Health and Social Care. The views are not a substitute for professional medical advice.