What is the evidence for mass gatherings during global pandemics?
March 20, 2020

David Nunan, John Brassey
On behalf of the Oxford COVID-19 Evidence Service Team
Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences
University of Oxford
Trip Database
Correspondence to david.nunan@phc.ox.ac.uk
Mass gatherings and sporting events during a pandemic PDF to download
VERDICT
The effect of restricting and cancelling mass gatherings and sporting events on infectious diseases is poorly established and requires further assessment. The best-available evidence suggests multiple-day events with crowded communal accommodations are most associated with increased risk. Mass gatherings are not homogenous and risk should be assessed on a case-by-case basis.
BACKGROUND
We previously reviewed the evidence for social distancing[1] in our COVID-19 Evidence Service. Here we take a closer look at the evidence for mass gatherings and sporting events and their impact on health and infectious disease in particular.
What is a mass gathering?
The World Health Organisation (WHO) describes a mass gathering as “a planned or spontaneous event where the number of people attending could strain the planning and response resources of the community or country hosting the event.”[2] The Olympic Games, The Hajj, and other major sporting, religious, and cultural events are all examples of a mass gathering.
What countries have restricted or banned mass gatherings due to COVID-19?
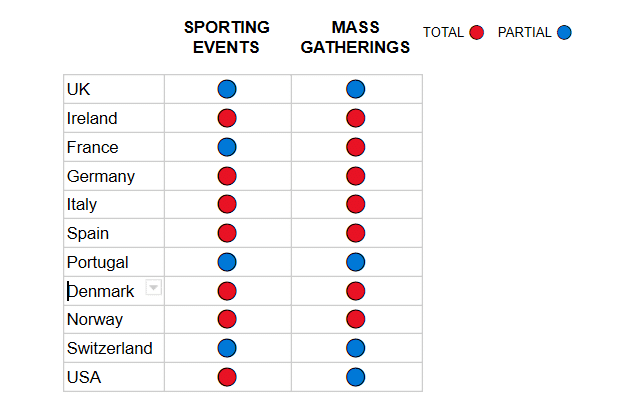
Table 1 provides a list of restrictions on mass gatherings and sporting events for selected countries (as of 17 March). It is clear that countries have varied in their approaches and timing of their adoption around mass gatherings and sporting events. Organisations responsible for mass events and sporting bodies have also taken decisions to either ban or postpone events even when government advice was advisory or absent (voluntary event cancellation [VEC])[2]; including the London Marathon, national soccer leagues and international tournaments, Formula 1, The Six Nations, World Tennis Association/Association of Tennis Professionals, Glastonbury festival and numerous national and local sporting, cultural and religious events. At the time of writing there has been no decision as to postponing the 2020 Tokyo Olympic games.
Table 1. Policy on restrictions for sporting events and mass gatherings in selected nations (as of 17 March)
 Sources:
Sources:
https://www.thesun.co.uk/news/11180796/coronavirus-countries-around-world-lockdown/ (accessed 17 March 2020)
https://www.pharmaceutical-technology.com/news/coronavirus-a-timeline-of-how-the-deadly-outbreak-evolved/ (accessed 17 March 2020)
CURRENT EVIDENCE
What is the evidence for mass gatherings and COVID-19?
At present evidence to answer this question comes almost solely from case reports, including incidences of outbreaks on cruise ships,[3] as well as a report of the first case of COVID-19 in Latin America coinciding with the Carnival.[4] Cruise ship conditions appear to have amplified the transmission of the disease. It is premature to speculate if this first case had sufficient contact with persons who attended the carnival or if the virus was already present in Brazil. There are multiple anecdotal reports but these lack data to verify.
A preprint article posted to medRxiv on 16 March performed a preliminary modeling analysis of VEC as a countermeasure against the COVID-19 outbreak in Japan during the period 26 February to 11 March.[5] The main outcome was change in the infectiousness of the disease based on the basic reproduction number [R0]. Results suggest that infectiousness of the disease was reduced by 25% (from R0 2.5 [95% CI; 2.43, 2.55] before VEC to 1.88 [1.68, 2.02] after). However, the methods and data have not been verified by peer review and should not be used to guide practice. As an example, the authors report a “35%” reduction in infectiousness which is most likely an error.
What impact do mass gatherings have on the transmission of infectious diseases?
While there is little evidence in relation to COVID-19 and mass gatherings there is the potential to extrapolate findings, judiciously, from other acute infectious diseases.
A key concern with mass gatherings is the increased risk of transmission of contagious infections as a result of large numbers of people in close contact for extended periods of time.[6]
Acute respiratory infections (ARI) appear to be the most common infectious disease transmitted during mass gatherings, particularly in the case of religious events. A recent systematic review of 45 studies assessed the impact of religious (n=15), sporting (n=17), festival (n=11) and other (n=4) gatherings. 10/15 studies of religious gatherings reported ARI as the most common infectious disease.[7] In the few studies assessing infectious diseases at sporting events (6/16), ARI was again the most common (but was second to trauma/injury across 16 studies). In studies of illness and infections at festivals (music, art), ARI were less commonly reported (2/11 studies).
A cross-sectional study of international mass gatherings using data from a global surveillance network of travel-related morbidity reported 296 ill travellers, the majority from religious (243 cases, 82.1%) but also cultural (e.g., music, dance, carnival) (19 cases; 6.4%), the World Scout Jamboree (17 cases; 5.7%), major sporting events (13 cases; 4.4%), and a large conference (4 cases; 1.4%).[8] Illness was directly associated with mass gathering attendance in 260 cases reporting a total of 303 diagnoses; ARI being the most frequently reported diagnosis (236 cases, 77.9%).
In a specific study of Indian pilgrims attending Hajj between 2014-2016, approximately 50.4% (50.3% to 50.6%) of all reported outpatient diagnoses were ARI, by far the most common diagnoses.[9]
A retrospective study in 273 French pilgrims attending the Hajj in 2009 reported a 2.3 fold increase in the incidence of influenza-like-illness (ILI) compared to a non-attending control (mean incidence of 1211 cases per 100,000 pilgrims versus 520 among a French Provence population).[10] The majority of pilgrims were vaccinated for seasonal flu but only a lower proportion (5.8%) were vaccinated against H1N1 pandemic influenza compared with the control population (11.7%).
Outbreaks of respiratory disease resulting from mass gatherings may be infrequent. A systematic review of mass gathering-related respiratory disease outbreaks occurring in the United States found them to be relatively rare (72 outbreaks over a 10-year period).[11] These findings need to be interpreted in their context of local and national events in a single nation.
Is the impact the same for different types of event?
A survey study of mass gatherings in the United States reporting on 18 respiratory-disease outbreaks between 2009-2016 found that more than half (61%) occurred at agricultural fairs in 2012 via zoonotic transmission.[12] Sporting, professional conferences, and religious events contributed only one reported outbreak each. The most common pathogen (n=11) was influenza A H3NSv from agricultural events (probable swine flu exposure), with various other influenza A pathogens forming the remaining. None of the reported outbreaks involved single-day mass gatherings, which reflected findings from the previous systematic review.[11]
A systematic review of 24 studies found evidence related to mass gatherings and influenza transmission to be sparse but available studies consistently demonstrate influenza transmission occurs amongst pilgrims at major religious events.[13] Major sporting events such as the Olympics and the soccer World Cup detected only marginal increased the incidence of all infectious diseases including influenza, with infections primarily limited to competitors and staff rather than crowds attending or the wider community. The evidence for large music festivals was “variable”.
Taken together, the best-available evidence points to influenza outbreak and transmission being influenced by the type of event, with key factors being the degree of crowdedness, the event duration and, possibly, whether the event is held indoors or outdoors. Multiple-day events with crowded communal accommodations may be the links to mass gatherings most associated with influenza.
What impact do restrictions have on the transmission of infectious diseases and does timing matter?
A large proportion of research in this area comprises modelling studies. Archival studies of the 1918-19 influenza pandemic in the United States imply that restricting mass gatherings was beneficial, particularly when implemented early. One study reported the early application of public gathering bans (concurrent with school closures) in 34/43(79%) cities was associated with greater delays in reaching peak mortality (r = -0.74, P < 0.001), lower peak mortality rates (r = 0.31, P = .02) and lower total mortality (r = 0.37, P = .008).[14] These findings, however, conflict with those from a study examining the pandemic’s impact in New York City. Other interventions were favoured over the banning of mass gatherings. New York reported one of the lowest excess death rates of any city during the pandemic.[15]
A related issue is ARI associated with travel and mass gatherings. Reductions of as much as 12% in peak ILI and delays of 1-1.5 weeks when >50% mean reduction in travel frequency have been modelled.[16] When modelled specifically to mass gatherings, those occurring 10 days before the epidemic peak can result in a 10% relative increase in peak influenza prevalence and total rate.[17] Conversely, mass travelling and gatherings may have little effect when occurring more than 40 days or 20 days later than the epidemic peak (when initial R0 = 1.5)
The cross-sectional study already cited indicates most reported illnesses, including ARI, are linked with travel but not actual attendance at the Olympics.[8] Most reported illnesses were mild and may reflect important differences between sporting and other mass events including physical separation, the propensity to hold the Olympics in high-income countries, the relatively short travel duration of attendees and participants, and the relatively young age of participants.
Limitations and considerations
Much of the evidence includes data derived from retrospective observational studies utilising questionnaire-based surveys, with little laboratory confirmation of diagnoses. The significance of mass gatherings to disease transmission is directly linked to the efficiency in transmission of the given virus. The R0 for COVID-19 has been estimated between 2.24-3.58.[18] The potential effectiveness of any public policy on mass gatherings includes the whole range of factors affecting adherence and compliance. Finally, mass gatherings are not homogenous and the risk should be assessed on a case-by-case basis.[19] All this must be taken into account when making decisions regarding mass gatherings in relation to COVID-19.
CONCLUSIONS
- Global data on COVID-19 continue to be collected. They must be actively analysed and used to support real-time decision making. However, until this evidence base grows, current COVID-19 policies may rely on inferences from other scenarios, such as influenza pandemics
- The effect of restricting and cancelling mass gatherings and sporting events on respiratory disease rates during pandemics in general is poorly established and requires further assessment
- Although limited; the best-available evidence appear to suggest multiple-day events with crowded communal accommodations are most associated with increased risk of transmission of respiratory infections
- The timing of restrictions on mass gatherings appears important; restrictions closer to epidemic peak may be more effective than restrictions applied further out
- Mass gatherings are not homogenous and risk should be assessed on a case-by-case basis.
Disclaimer: the article has not been peer-reviewed; it should not replace individual clinical judgement and the sources cited should be checked. The views expressed in this commentary represent the views of the authors and not necessarily those of the host institution, the NHS, the NIHR, or the Department of Health and Social Care. The views are not a substitute for professional medical advice.
Authors
 David Nunan is a Senior Research Fellow at the Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences, University of Oxford. He is also an Editor at the BMJ Evidence-Based Medicine journal and Director of PG Certificate in Teaching Evidence-Based Health Care
David Nunan is a Senior Research Fellow at the Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences, University of Oxford. He is also an Editor at the BMJ Evidence-Based Medicine journal and Director of PG Certificate in Teaching Evidence-Based Health Care
@dnunan79
Jon Brassey is the Director of Trip Database Ltd, Lead for Knowledge Mobilisation at Public Health Wales (NHS) and an Associate Editor at the BMJ Evidence-Based Medicine
Evidence search
We searched the Trip Database, Google Scholar and PubMed using the following terms:
“mass gatherings” AND (“bronchitis” OR “common cold” OR “influenza” OR “pneumonia” OR “SARS” OR “MERS” OR “acute respiratory infections” OR “severe respiratory infections” OR “coronavirus”) for primary studies or systematic reviews. We also performed citation analysis of relevant articles.
References
1 World Health Organisation (WHO). What is WHO’s role in mass gatherings? https://www.who.int/news-room/q-a-detail/what-is-who-s-role-in-mass-gatherings (accessed 16 March 2020)
2 UK to ban mass gatherings in coronavirus U-turn. Guardian online 13 March 2020. (accessed 16 March 2020)
3 Rocklöv J, Sjödin H, Wilder-Smith A. COVID-19 outbreak on the Diamond Princess cruise ship: estimating the epidemic potential and effectiveness of public health countermeasures, Journal of Travel Medicine, taaa030. doi.org/10.1093/jtm/taaa030
4 Rodriguez-Morales A J, Gallego Viviana, Escalera-Antezana J P et al. COVID-19 in Latin America: The implications of the first confirmed case in Brazil. Travel Medicine and Infectious Disease. In Press. doi.org/10.1016/j.tmaid.2020.101613
5 Sugishita Y, Kurita J, Sugawara T, Ohkusa Y. Preliminary evaluation of voluntary event cancellation as a countermeasure against the COVID-19 outbreak in Japan as of 11 March, 2020. medRxiv 2020.03.12.20035220. doi.org/10.1101/2020.03.12.20035220
This article is a preprint and has not been peer-reviewed [what does this mean?]. It reports new medical research that has yet to be evaluated and so should not be used to guide clinical practice.
6 Memish ZA, Steffen R, White P, et al. Mass gatherings medicine: public health issues arising from mass gathering religious and sporting events. Lancet 2019; 393: 2073–84
7 Karami M, Doosti-Irani A, Ardalan A, et al. Public Health Threats in Mass Gatherings: A Systematic Review. Disaster Med Public Health Prep. 2019;13(5-6):1035–1046. doi:10.1017/dmp.2018.161
8 Javelleo E, Mendelson M, Glansq H, et al. International mass gatherings and travel-associated illness: A GeoSentinel cross-sectional, observational study. Travel medicine and infectious disease. 2019;32:101504. doi.org/10.1016/j.tmaid.2019.101504
9 Khan ID, Khan SA, Asimac B, et al. Morbidity and mortality amongst Indian Hajj pilgrims: A 3-year experience of Indian Hajj medical mission in mass-gathering medicine. Journal of infection and public health. 2018; 11(2):165-170
10 Gautretab P, Parolaab P, Brouquiab P. Relative risk for influenza like illness in French Hajj pilgrims compared to non-Hajj attending controls during the 2009 influenza pandemic. Travel medicine and infectious disease. 2013;11(2):95-7
11 Rainey JJ, Phelps T, Shi J. Mass Gatherings and Respiratory Disease Outbreaks in the United States – Should We Be Worried? Results from a Systematic Literature Review and Analysis of the National Outbreak Reporting System. PLoS ONE. 2016;11(8): e0160378. doi.org/10.1371/journal.pone.0160378
12 Figueroa A, Gulati RK, Rainey JJ. Estimating the frequency and characteristics of respiratory disease outbreaks at mass gatherings in the United States: Findings from a state and local health department assessment. PLoS One. 2017;12(10):e0186730. doi:10.1371/journal.pone.0186730
13 Isholaab DA, Phinac N. Could influenza transmission be reduced by restricting mass gatherings? Towards an evidence-based policy framework. Journal of epidemiology and global health 2011; 1(1):33-60
14 Markel H, Lipman HB, Navarro JA, et al. Nonpharmaceutical Interventions Implemented by US Cities During the 1918-1919 Influenza Pandemic. JAMA. 2007;298(6):644–654. doi:10.1001/jama.298.6.644
15 Aimone, F. The 1918 Influenza Epidemic in New York City: A Review of the Public Health Response. Public Health Reports. 2010;125(3_suppl):71–79. doi.org/10.1177/00333549101250S310
16 Bolton KJ, McCaw JM, Moss R, et al. Likely effectiveness of pharmaceutical and non-pharmaceutical interventions for mitigating influenza virus transmission in Mongolia. Bull World Health Organ. 2012;90(4):264–271. doi:10.2471/BLT.11.093419
17 Shi, P., Keskinocak, P., Swann, J.L. et al. The impact of mass gatherings and holiday traveling on the course of an influenza pandemic: a computational model. BMC Public Health 10, 778 (2010). doi.org/10.1186/1471-2458-10-778
18 Chih-Cheng Laia, Tzu-Ping Shih, Wen-Chien Ko. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. International Journal of Antimicrobial Agents. 2020: 55(3):105924 doi.org/10.1016/j.ijantimicag.2020.105924
19 Risk-informed decision-making for mass gatherings during COVID-19 global outbreak. https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/health-professionals/mass-gatherings-risk-assesment.html (accessed 18 March 2020)