More about chloroquine and hydroxychloroquine
May 30, 2020
Updated 30 August 2020 and 28 July 2021
Jeffrey K Aronson, Robin E Ferner*†
On behalf of the Oxford COVID-19 Evidence Service Team
Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences,
University of Oxford
*University of Birmingham
†University College London
Correspondence to jeffrey.aronson@phc.ox.ac.uk
VERDICT
The hypothesis that the 4-aminoquinolines chloroquine and hydroxychloroquine may be beneficial in the treatment of COVID-19 is a weak one, based on poor mechanistic reasoning and inconsistent results of studies in vitro, in laboratory animals, and in humans.
The risks of adverse reactions to these drugs may be increased in patients who are acutely ill with severe COVID-19, in many of whom high doses are being used.
Macrolide antibacterial drugs, such as azithromycin, clarithromycin, erythromycin, and telithromycin, interact adversely with the 4-aminoquinolines, since both types of drug prolong the electrocardiographic QT interval. The combination increases the risk of the serious ventricular tachycardia called torsades de pointes, which is often fatal. Macrolide antibacterial drugs should be avoided in patients taking chloroquine or hydroxychloroquine. Other drugs that prolong the QT interval should also be avoided or used with care.
The latest evidence suggests that mortality may be increased by hydroxychloroquine in individuals with severe covid-19, and current advice is a strong contraindication against using it.
BACKGROUND
We have previously expressed concerns about the widespread use of the 4-aminoquinolines chloroquine and hydroxychloroquine in the treatment of COVID-19. Our reasons were as follows:
- The hypothesis that they should affect viral growth in COVID-19 is based on weak evidence from other viral infections in vitro, in animals, and in clinical studies.
- Similarly, the likelihood of benefit, based on poor mechanistic reasoning, is small.
- The high doses of the 4-aminoquinolines that are being used in COVID-19 increase the risk of adverse drug reactions.
- Drug–drug interactions can occur, for example between the 4-aminoquinolines and the macrolide antibacterial drug azithromycin, with which the drugs have often been used in combination.
1. Weak evidence for the hypothesis of efficacy
In cell cultures and animal studies, the effects of 4-aminoquinolines on viruses from avian influenza virus (H5N1) to Zika have been inconsistent.
- In some laboratory experiments the drugs have inhibited viral growth. But in a study in cells infected by Epstein-Barr virus chloroquine increased viral replication.
- In an in vivo study, chloroquine reduced transmission of Zika virus to the offspring of five infected mice. However, while chloroquine inhibited Ebola virus replication in vitro, it caused rapid worsening of Ebola infection in guinea pigs and made no difference to mortality in mice or hamsters.
- In chikungunya virus infection, chloroquine was active in laboratory studies but it worsened the clinical course of infection in macaque monkeys.
Translation of beneficial effects from animals to humans has also been inconsistent. For example, chloroquine inhibited dengue virus in some cell cultures but failed to shorten the illness in a randomized study of 37 patients, although it improved some symptoms. And although laboratory studies suggested activity against influenza virus, chloroquine did not prevent infection in a large randomized trial.
Such inconsistent laboratory and clinical evidence is partly due to the complex pharmacokinetics of 4-aminoquinolines, both chloroquine and hydroxychloroquine, making it difficult to extrapolate from cell culture experiments to human use and difficult to find satisfactory dosages during an acute infection.
The null hypothesis to be tested is that the 4-aminoquinolines are not efficacious in COVID-19. The past failures give no confidence in the alternative hypothesis, namely that these drugs will benefit patients with COVID-19, or indeed any new acute viral infection.
2. Small likelihood of benefit
The mechanism of action of the 4-aminoquinolines is not known, despite many years of use as antiplasmodial drugs in malaria and in conditions such as rheumatoid arthritis and systemic and discoid lupus erythematosus. The most commonly cited hypothesis for their antiviral action is that they are weak bases and increase endosomal pH in host intracellular organelles, inhibiting autophagosome-lysosome fusion and inactivating enzymes that viruses require for replication. They may also affect glycosylation of angiotensin converting enzyme-2 (ACE-2), the receptor that SARS-CoV-2 uses as one of two mechanisms to enter cells; there is no evidence that they alter the viral membrane fusion mechanism.
However, even if these mechanisms are relevant to SARS-CoV-2, the 4-aminoquinolines are unlikely to do more than partially reduce viral invasion of cells and intracellular replication, not abolish it completely. At best this might be expected to delay the onset of the illness and perhaps shorten its duration.
Our previous concerns were borne out by the results of early clinical studies, which showed either little or no beneficial effect. However, these studies were generally small and of poor quality, and mortality was not a primary outcome. The results of properly masked randomized controlled trials were awaited, and still are.
3. The risk of adverse drug reactions
It is often claimed that we know all about how safe the 4-aminoquinolines are, because they do not often cause serious adverse reactions when they are used for their licensed indications, and are therefore unlikely to cause serious adverse reactions when used to treat acute viral infections. This is an unjustifiable assumption, for two reasons.
First, there is no guarantee that, because a drug is safe at one dose, it will be safe at a higher dose. The Summary of Product Characteristics (SmPC) for Plaquenil (hydroxychloroquine sulfate, Zentiva) recommends that the dose should not exceed 6.5 mg/kg/day and will be either 200 or 400 mg/day. The adult dosage regimen in the RECOVERY trial is 2400 mg in the first 24 hours followed by 400 mg 12-hourly for 10 days or until discharge from hospital, which could be longer. In 45 registered trials of hydroxychloroquine in COVID-19 for which enough information is given for calculations to be made, the average daily dose over the period of treatment is over 400 mg and in some as high as 1200 mg/day.
Secondly, the absence of serious adverse reactions during treatment of a chronic condition is no guarantee of freedom from adverse reactions when treating an acute severe infection. For example, the 4-aminoquinolines can rarely cause seizures and so can COVID-19. We do not know if the risk of drug-induced seizures is therefore increased when the drugs are used to treat COVID-19.
4. The risk of drug-drug interactions
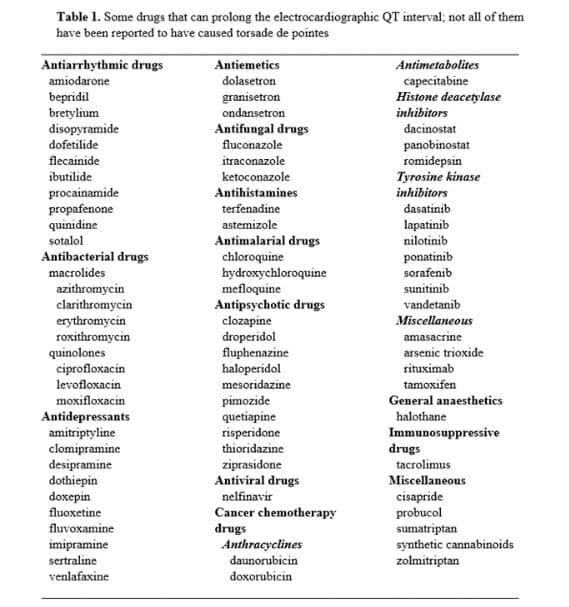
The 4-aminoquinolines prolong the electrocardiographic QT interval. This effect is exacerbated when they are used in combination with other drugs that prolong the QT interval. The SmPC for Plaquenil warns against using hydroxychloroquine in combination with other arrhythmogenic drugs.
Many drugs, and not just antiarrhythmic drugs, can prolong the QT interval (Table 1). Among them are the macrolide antibiotics, azithromycin, clarithromycin, erythromycin, roxithromycin, and telithromycin. The risk is increased when drugs that prolong the QT interval are used in combination, as has been reported in several studies when hydroxychloroquine and azithromycin have been combined.
When the QT interval is prolonged in this way there is an increased risk of the polymorphous ventricular tachycardia called torsades de pointes, which can be fatal. The risk of torsades de pointes is increased in the presence of hypokalaemia, to which patients with COVID-19 are susceptible. The risk of azithromycin-induced prolongation of the QT interval is also increased in elderly people, who are at increased risk of developing severe COVID-19, and in patients in intensive care units, where they are likely to be treated.
Several studies of the combination of azithromycin + hydroxychloroquine in COVID-19 have shown an increased risk of cardiac arrhythmias.
A recent registry study of data from 671 hospitals worldwide in more than 96,000 patients with COVID-19, of whom 16% been treated with a 4-aminoquinoline, reported that mortality was 7530/81144 (9%) in patients who received neither drug and 3168/14888 (21%) in those who received either chloroquine or hydroxychloroquine; those who received azithromycin or clarithromycin in addition to a 4-aminoquinoline were at higher risk of dying (2318/10004, 23%) than those who received a 4-aminoquinoline alone (850/4884, 17%). Worrying though these data are, they do not constitute definitive evidence of an unfavourable benefit to harm balance, since treatments were not randomly allocated and confounding could have occurred. Furthermore, since the data were published doubt has been cast on their provenance and accuracy, which await confirmation.
Note added on 4 June: The authors have now retracted their paper. They were unable to complete an independent audit of the data underpinning their analysis and have therefore concluded that they “can no longer vouch for the veracity of the primary data sources.” The retraction notice can be found at https://www.thelancet.com/lancet/article/s0140673620313246/.
Current trials involving the 4-aminoquinolines
The World Health Organization has temporarily halted the hydroxychloroquine arm of its Solidarity trial, pending analysis of the data so far obtained. The Oxford-based PRINCIPLE trial in UK general practices also suspended the hydroxychloroquine arm, the trial continues to evaluate other drugs. The Oxford–Brighton COPCOV study has been halted, under guidance from the UK regulator, the Medicines and Healthcare products Regulatory Agency (MHRA), as reported in the medical press. At the same time, the MHRA has reportedly said that it agrees with a statement from the investigators of the Oxford-led RECOVERY trial, that “the data [analysed by an independent committee] provide reassurance that continued enrolment into the hydroxychloroquine arm is safe and that we should press ahead with getting a reliable answer on hydroxychloroquine”.
Note added on 5 June: The data on the use of hydroxychloroquine in the RECOVERY trial have now been more fully analysed: 1542 patients were randomized to hydroxychloroquine and compared with 3132 patients randomised to usual care alone. There was no significant difference in the primary endpoint of 28-day mortality (25.7% hydroxychloroquine vs. 23.5% usual care; hazard ratio 1.11 [95% confidence interval 0.98-1.26]; P=0.10). Nor was there evidence of beneficial effects on hospital stay duration or other outcomes. The investigators concluded that “These data convincingly rule out any meaningful mortality benefit of hydroxychloroquine in patients hospitalised with COVID-19.” Indeed the data show a trend towards increased mortality in those given hydroxychloroquine, since the lower 95% confidence bound for the hazard ratio is only just below 1. They have stopped enrolling patients into the hydroxychloroquine arm of the trial.
Note added on 27 June: On 26 June the MHRA announced that it had “given the [COPCOV] clinical trial the green light to recruit more participants at the request of the COPCOV trialists, who are studying the use of hydroxychloroquine in preventing COVID-19. At the same time, the MHRA issued a statement reminding prescribers that “Chloroquine and hydroxychloroquine are not licensed to treat COVID-19 related symptoms or prevent infection” and that “until we have clear, definitive evidence that these treatments are safe and effective for the treatment of COVID-19, they should only be used for this purpose within a clinical trial.”
Update added on 30 August 2020
Since we last updated this vignette, the first iteration of a “living”—a frequently updated—meta-analysis of trials of treatment for covid-19, a very large international collaborative project, co-ordinated from McMaster University, has been published in the BMJ. The conclusion was that “So far no convincing evidence indicates that any treatments [other than dexamethasone] have a benefit for mortality when compared to standard care or each other. The main limitations of the evidence across comparisons are risk of bias and imprecision.”
The data on hydroxychloroquine, with mostly low degrees of certainty, showed no change in mortality, no change in the time to viral clearance, a small reduction in the time to symptom resolution (from 19 to 14.5 days) and a large significant increase in the risk of adverse events (from 15 per 1000 to 985 per 1000).
A “living” series of systematic reviews of various pharmacological interventions, co-ordinated from Paris, is also available online, and a protocol for another such review has been published. Several other systematic reviews have been published, but none of those that we have seen to date have excluded observational studies of various kinds.
The randomized controlled data on hydroxychloroquine are dominated by the (preliminary) results of RECOVERY. We have discussed this trial above, but it was not included in the McMaster meta-analysis, which included only smaller randomized trials of chloroquine or hydroxychloroquine. The results of RECOVERY are judged to be reliable, although “some concerns” were noted in the French systematic review over the potential for bias from the lack of masking and from the decision by the Data Monitoring Committee to recommend that the data be reported early. That decision was to be expected, as RECOVERY was an adaptive trial.
The following results of randomized trials of hydroxychloroquine in established covid-19 and in post-exposure prophylaxis have been published. We have not included observational studies nor systematic reviews that included such studies.
Huang et al (J Mol Cell Biol, 1 April 2020)
A small randomized Chinese study reported the outcomes in SARS-CoV-2-positive patients, 10 of whom were treated with chloroquine (10 g over 10 days) and 12 with lopinavir–ritonavir. None of the measures of outcome was statistically significant. This study was not powered to detect even the difference in vomiting between the chloroquine group (5/10) and the lopinavir–ritonavir group (1/12) (P = 0.06).
Borba et al (JAMA, 24 April 2020)
In a masked, randomized study from Brazil, patients with suspected severe covid-19 were randomized to low-dose or high-dose chloroquine (2.7 g over 5 days or 12 g over 10 days). The study was halted early, on the advice of the Data Safety Monitoring Committee. The primary endpoint was mortality at 28 days. Patients in the high-dose group were older and more had cardiac disease. After 81 patients had been recruited, 16/41 in the high-dose group and 4/40 in the low-dose group had died (OR = 3.6; 95% CI = 1.2–10.6). The QTc interval was above 500 ms in 7/37 patients in the high-dose group and 4/36 in the low-dose group. Ventricular tachycardia occurred in two patients in the high-dose group before they died. There were no recorded cases of ventricular tachycardia in the low-dose group. Treatment with chloroquine 12 g given over 10 days was not safe, as the authors stated. There was no evidence that the lower dose was effective.
Tang et al. (BMJ, 14 May 2020)
A second report from China detailed a multicentre, unmasked, randomized controlled trial, in which hydroxychloroquine (1200 mg/day for 3 days followed by 800 mg/day for 2–3 weeks) was compared with standard care in 150 hospitalized patients with covid-19, 148 with mild to moderate disease and two with severe disease. The probability of negative conversion by 28 days did not differ between the two groups. Adverse events were more common with hydroxychloroquine (30% versus 9%).
Boulware et al (N Engl J Med, 3 June 2020)
In a randomized, double-blind, placebo-controlled trial of hydroxychloroquine as postexposure prophylaxis, 821 asymptomatic adults who had had household or occupational exposure to someone with confirmed covid-19 at a distance of less than 6 ft for more than 10 minutes while wearing neither a face mask nor an eye shield (high-risk exposure; n = 719) or while wearing a face mask but no eye shield (moderate-risk exposure) were randomized within 4 days after exposure to either placebo or hydroxychloroquine (800 mg, 600 mg 6-8 h later, then 600 mg/day for 4 days. Hydroxychloroquine did not prevent illness compatible with covid-19 or confirmed infection compared with placebo. Adverse events were more common with hydroxychloroquine than with placebo (40% versus 17%), but no serious adverse events were reported.
Chen et al (medRxiv, 22 June 2020)
In an unmasked Chinese randomized controlled trial, published in preprint, 12 patients given standard care alone were compared with 36 treated with 4-aminoquinolines: 18 with chloroquine (5.5 g over 10 days) and 18 with hydroxychloroquine (4 g over 10 days). All had covid-19 of moderate intensity; those in the standard care arm were on average five years older than those in the 4-aminoquinoline arms. Viral RNA tests became negative more rapidly in those treated with 4-aminoquinolines, and pairwise comparisons with standard care suggested a more rapid clinical improvement in the actively treated patients, nearly half of whom reported adverse effects of treatment. This was a small unmasked trial that recruited only 48 patients, half the intended number. An initial demonstration that there were significant differences among the three arms would have made the pairwise comparisons more secure.
Davoodi et al. (Int J Clin Pract, 30 June 2020)
In an Iranian unmasked randomized comparison of febuxostat 80 mg/day and hydroxychloroquine 200 mg bd for 5 days in 60 adult outpatients with moderate respiratory disease after covid-19 infection, the effects on fever, cough, and tachypnoea were the same in the two groups. In the absence of a placebo comparison, nothing can be concluded from the results of this study.
Skipper et al (Ann Intern Med, 16 July 2020)
A North American randomized, masked, placebo-controlled trial examined outcomes in 423 of 491 mildly symptomatic outpatients with laboratory confirmed covid-19 “or epidemiologically linked exposure to a person with laboratory-confirmed infection”, who were given hydroxychloroquine (800 mg once, then 600 mg 6–8 hours later, then 600 mg once daily for 4 more days) or placebo. The primary outcome measure was a change at 14 days in symptoms measured on a 10-point visual analogue scale of severity. There was a non-significant benefit of –0.27 points (95% CI = –0.61 to 0.07). Symptoms were present at 14 days in 49/201 patients treated with hydroxychloroquine and 59/194 treated with placebo. One patient in each group died. Patients treated with hydroxychloroquine reported adverse events at five days twice as often as those in the placebo group: 92/203 (43.4%) versus 46/194 (21.8%) (OR = 2.67; 95% CI = 1.7 to 4.1). This result appears to offer a choice between symptoms of covid-19 and symptoms of the adverse effects of hydroxychloroquine, although a small benefit cannot be excluded.
Mitjà et al (Clin Infect Dis, 16 July 2020)
In a multicentre, unmasked, randomized, controlled trial in Catalonia, 293 non-hospitalized adults with SARS-CoV-2 infection and under five days of symptoms were randomized to hydroxychloroquine (800 mg on day 1, followed by 400 mg/day for 6 days) or no antiviral treatment (not placebo-controlled). There were no significant benefits on risk of hospitalization (RR = 0.75; 95% CI = 0.32-1.77) or time to complete resolution of symptoms; there were no relevant treatment-related adverse events. The trial was small, with wide confidence intervals for the outcomes.
Mitjà et al (SSRN, 16 July 2020)
In an unmasked, randomized, prospective, cluster-controlled trial in three health regions in Catalonia, non-hospitalized adult patients SARS-CoV-2 infection and under seven days of symptoms were randomized to hydroxychloroquine (800 mg on day 1, followed by 400 mg/day for 6 days) plus darunavir/cobicistat (800/150 mg/day for seven days; n = 165) or no antiviral treatment (n = 142). No benefits were seen on viral load or time to complete alleviation of symptoms.
Mitjà et al (MedRxiv, 26 July 2020)
The same Spanish group published a preprint of an unmasked, cluster-randomized trial of the efficacy of hydroxychloroquine (800 mg on day 1, followed by 400 mg/day for 6 days) or placebo in 2314 asymptomatic contacts of patients who had tested for SARS-CoV-2. Clusters were defined as “rings” – groups of healthy contacts who were linked to a PCR-positive case of covid-19. The results were adjusted to account for clustering within rings. There were 338 clusters in the treatment arm and 334 in the control arm. The rates of subsequent PCR-confirmed symptomatic covid-19 were 6.2% usual care and 5.7% hydroxychloroquine (risk ratio = 0.89; 95% CI = 0.54–1.46). Adverse events were reported in 52% of treated patients and 5.9% of control patients. Deaths were commoner in the control arm (8/1300) than the treatment arm (5/1197). The study design, derived from studies on Ebola, is attractive. The results do not suggest that post-exposure prophylaxis with hydroxychloroquine will prevent symptomatic covid-19. However, the median time from exposure to enrolment was 4 days, so the study could not definitively exclude a benefit of earlier prophylaxis.
Cavalcanti et al (N Engl J Med, 23 July 2020)
A Brazilian group studied 667 hospital patients with suspected or confirmed covid-19 who did not require more than 4 L/min supplemental oxygen. Patients were randomly allocated to standard care, hydroxychloroquine (800 mg/day), or hydroxychloroquine (800 mg/day) + azithromycin (500 mg/day) for 7 days. The primary outcome was status on a seven-point ordinal scale, evaluated at 15 days after randomization. Neither the ordinal outcome at day 15 nor overall mortality differed significantly among the groups, analysed by intention to treat, whether or not the analysis was restricted to the 504 patients who tested positive for SARS-CoV-2. QTc interval longer than 480 ms was more than twice as common in those who received hydroxychloroquine, with or without azithromycin (15%), as in the control group (6%). There were three cases of supraventricular tachycardia in the hydroxychloroquine group. Raised liver enzymes were also more than twice as common in those exposed to hydroxychloroquine (10%) as in controls (4%). The authors concluded that “Among patients hospitalized with mild-to-moderate Covid-19, the use of hydroxychloroquine, alone or with azithromycin, did not improve clinical status at 15 days as compared with standard care.”
Abd-Elsalam et al (Am J Trop Med Hyg, 14 August 2020)
In an Egyptian multicenter, randomized, controlled trial, 194 patients with COVID-19 were given standard care with or without hydroxychloroquine (400 mg twice daily on day 1 followed by 200 mg twice daily for 15 days). Standard care included paracetamol, oxygen, an empirical antibiotic (a cephalosporin), and oseltamivir “if needed”. The primary endpoints, recovery within 28 days, the need for mechanical ventilation, and deaths, were not altered by adding hydroxychloroquine to standard care.
Conclusions
Many trials of the 4-aminoquinolines are currently being conducted globally. Many of them are unmasked, and many of them involve the use of high doses. It is therefore important to establish the benefit to harm balance in high-quality trials.
Patients who are given either chloroquine or hydroxychloroquine should not also be given any other medicines that prolong the QT interval. If such combinations are unavoidable, the electrocardiogram should be carefully monitored for evidence of QT interval prolongation.
Further conclusion added on 30 August 2020
We see no reason to alter the verdict with which we began this article when we wrote it in May this year. The latest data suggest that the harms from using the 4-aminoquinolines, chloroquine and hydroxychloroquine, to treat established covid-19 outweigh their benefits and that there is no benefit in post-exposure prophylaxis. Trials of pre-exposure prophylaxis have also been registered, e.g. ACTRN12620000417987, NCT04328467, NCT04331834, NCT04334928, and see also here.
Further update added on 28 July 2021
The REMAP-CAP Investigators (see also here) have recently reported further results. In a multicentre trial they randomly allocated 726 critically ill patients with covid-19 to one of four “antiviral domain interventions”. Of 694 patients analysed, 255 were allocated to lopinavir-ritonavir, 50 to hydroxychloroquine, 27 to the combination; 362 controls were given neither medication. Hydroxychloroquine was given as two loading doses of 800 mg, 6 hours apart, followed 6 hours later by 400 mg 12 hourly for 12 doses.
The outcomes were worse in the treated groups than in the controls. Specifically, the treated patients had significantly fewer support-free days and higher mortality rates.
The current advice from the living network meta-analysis of treatments for covid-19 published in the BMJ is as follows:
- Corticosteroids: Strong recommendation in favour in severe cases; weak recommendation against in mild to moderate cases
- IL-6 receptor blockers (e.g. tocilizumab): Strong recommendation in favour
- Hydroxychloroquine: Strong recommendation against
- Lopinavir-ritonavir: Strong recommendation against
- Ivermectin: Strong recommendation against (except in clinical trials)
- Remdesivir: Weak recommendation against
This advice is identical to that given by the WHO in its living guideline “Therapeutics and COVID-19.”