COVID 19 – Understanding the Unknown in Acute Respiratory Infections
May 11, 2020
Tom Jefferson, Carl Heneghan
As the shattered and half-frozen remnants of Napoleon’s once-mighty Grand Armee approached Vilnius in early December 1812 they saw in front of them the first undamaged walled city they had seen for many months.
Vilnius had ten gates. Officers had been deployed in front of the walls to direct the retreating columns to different assembly areas. The first in the column however made for the nearest entrance: the Gate of Dawn. This is a narrow tunnel-like defensive entrance which was swiftly choked by the press of half-crazed skeletal soldiers, carriages and artillery. Soon the gate was turned into a scene of horror, with scores of human beings literally crushed to death by the impetus of those behind them. The effects can be seen today in the corpses of those who perished.
Remarkably, those approaching the gate who could see what was going on, added to the press, with few seeking other gates. The long and harrowing retreat from Moscow had turned them into a herd of sheep, each following in the footsteps of the person in front of them.
Since the mid-1990s, we have been supposedly preparing for a pandemic. Much of the preparedness has been focussed on one agent, influenza – and herd thinking – despite two warnings: SARs-Co-V-1 and MERs
Massive amounts of resources have been invested in stockpiling specific treatments or preventive biologics which have never been properly tested and hardly used. Yet, their capacity to stop the spread of influenza is debatable.
Surveillance studies carried out in defined whole populations (usually nursing homes or student accommodation) over a defined time period have given us valuable insight into what is actually happening.
Proportional Incidence Epidemiology (PIE)
In a PIE study all participants or a truly random sample are swabbed (something routine surveillance cannot achieve). There is one other source of information that can help us, which is the control arms of formal studies on influenza vaccines and antivirals. Here again, the surveillance and follow-up are intensive following the protocol.
The figure below is a breakdown of pooled data from control arms in a suite of Cochrane reviews (1,200,000 observations from 356 datasets) and 59 datasets from pie studies (29,525 observations).
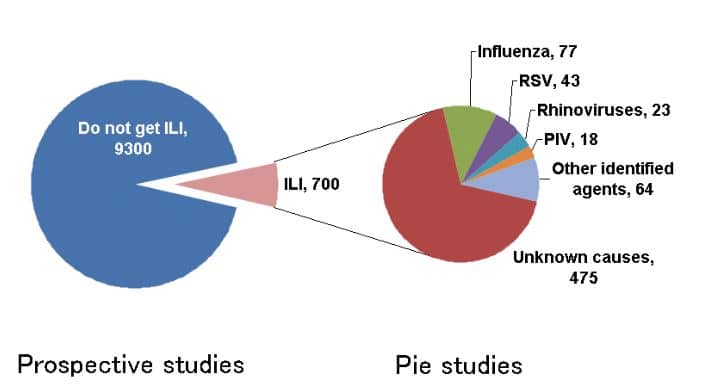
What this shows is that there are many more agents that cause Influenza-like illness (ILI).
If projected on a population of 10,000 of all ages, the incidence of ILI is 700/10000 and the lion share of agents are currently unknown.
The list of agents includes:
- Influenza (11%)
- Respiratory Syncytial Virus: RSV (6.1%)
- Rhinoviruses (3.3%)
- Parainfluenza viruses (2,5%)
- Other agents (9.1%). These likely to include metapneumoviridae, coronoviridae and echoviridae.
- Unknown (68~%)
In our article on RCGP surveillance, we noted that during the last week for which data are available (week 17 of 2020) out of 428 community samples, 353 (82.5%) were an unknown agent, and only 75 (17.5%) were positive for COVID 19.
Furthermore, several studies show there is a high proportion of viral infection in patients with community-acquired pneumonia. The WHO reports between 1.6 and 2.2 million deaths in under 5s occur because of acute respiratory infections: 40% of these are caused by viral infections. In both children and adults, CAP is caused by a variety of pathogens and in a proportion, the agent often remains unknown.
Several different sources show that a large proportion of pathogens implicated in respiratory infections are unknown. This could be because the ILI has no recognised agent, or mistakes in the sampling and testing have been made, or some may have a non-infectious cause.
This type of evidence generates uncertainties, but should also stimulate further research, broader thinking and a more flexible approach to pandemic preparedness.
Even the survivors of the retreat from Moscow might avoid the swinging certainties of our days.